Chen Jefferson W, Xu Jordan C, Malkasian Dennis, Perez-Rosendahl Mari A, Tran Diem Kieu
Department of Neurological Surgery, University of California, Irvine, Orange, CA, United States.
Neuropathology Division, Department of Pathology, University of California, Irvine, Orange, CA, United States.
Front Neurol. 2021 May 6;12:660885. doi: 10.3389/fneur.2021.660885. eCollection 2021.
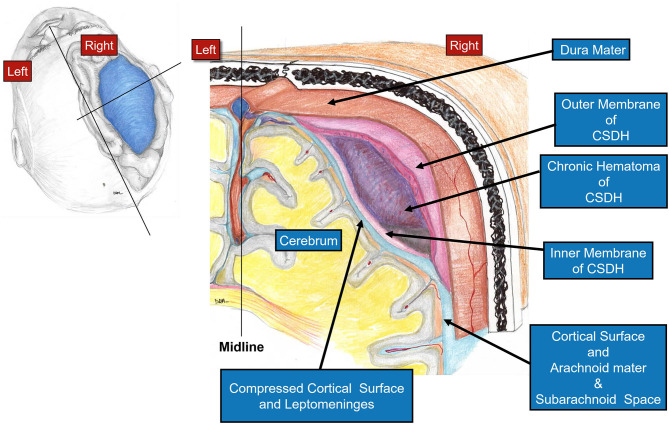
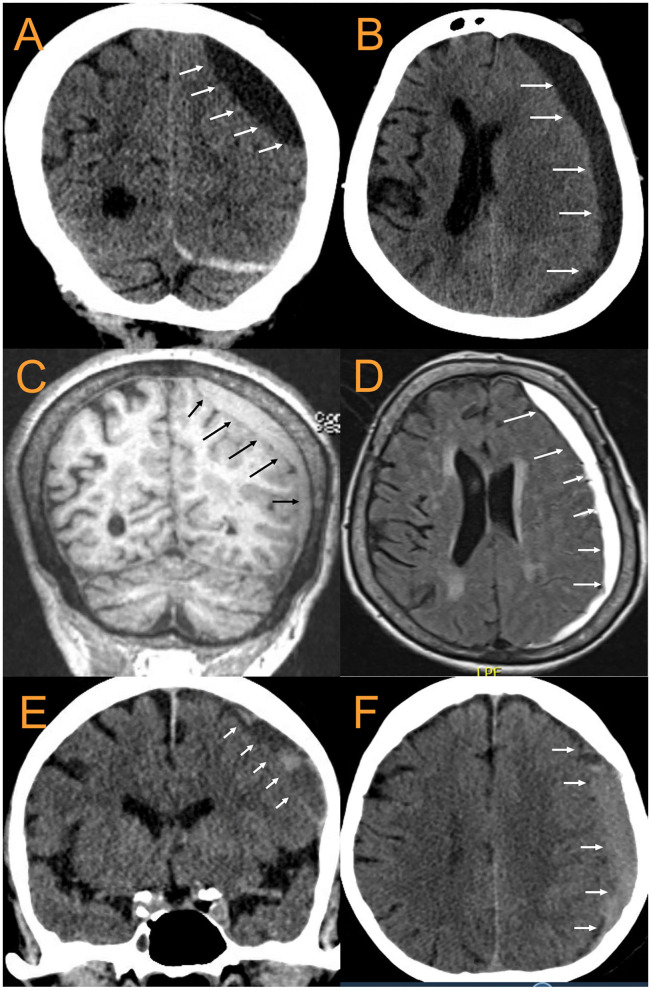
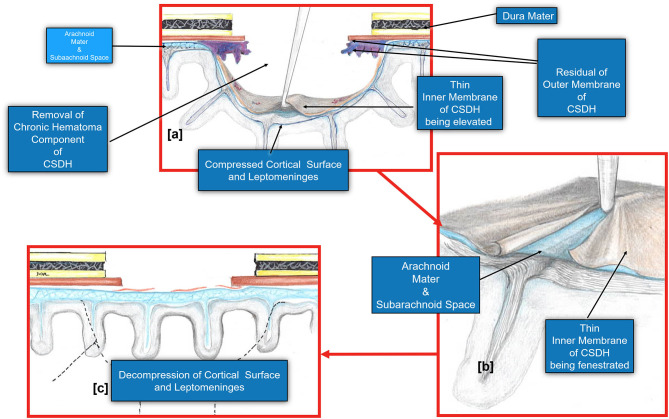
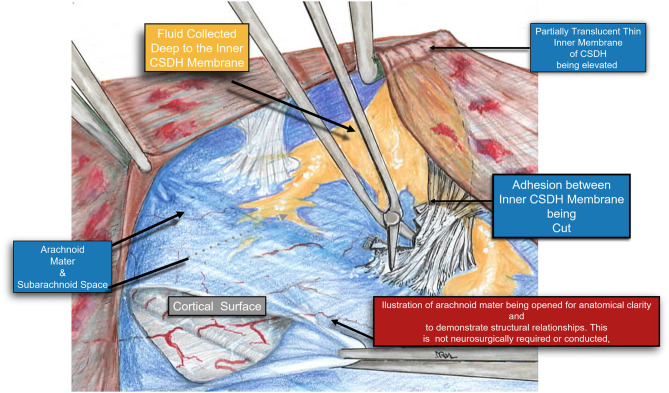
Chronic subdural hematomas (cSDH) are increasingly prevalent worldwide with the increased aging population and anticoagulant use. Different surgical, medical, and endovascular treatments have had varying success rates. Primary neurosurgical interventions include burr hole drainage of the cSDH and mini-craniotomies/craniotomies with or without fenestration of the inner membrane. A key assessment of the success or failure of cSDH treatments has been symptomatic recurrence rates which have historically ranged from 5 to 30%. Pre-operative prediction of the inner subdural membrane by CT scan was used to guide our decision to perform mini-craniotomies. Release of the inner membrane facilitates the expansion of the brain and likely improves glymphatic flow. Consecutive mini-craniotomies ( = 34) for cSDH evacuation performed by a single neurosurgeon at a quaternary academic medical center/Level I trauma center from July 2018-September 2020 were retrospectively reviewed. Patient characteristics [age, gender, presenting GCS, GOS, initial CTs noting the inner subdural membrane, midline shift (MLS), cSDH width, inner membrane fenestration, cSDH recurrence, post-operative seizures, infections, length of stay] were extracted from the EMR. Twenty nine patients had mini-craniotomies as primary treatment of the cSDH. Mean age = 68.9 ± 19.7 years (range 22-102), mean pre-operative GCS = 14.5 ± 1.1, mean MLS = 6.75 ± 4.2 mm, and mean maximum thickness of cSDH = 17.7 ± 6.0 mm. Twenty four were unilateral, five bilateral, 34 total craniotomies were performed. Thirty three had inner membrane signs on pre-operative head CTs and an inner subdural membrane was fenestrated in all cases except for the one craniotomy that didn't show these characteristic CT findings. Mean operating time = 79.5 ± 26.0 min. Radiographic and clinical improvement occurred in all patients. Mean improvement in MLS = 3.85 ± 2.69. There were no symptomatic recurrences, re-operations, surgical site infections, or deaths during the 6 months of follow-up. One patient was treated for post-operative seizures with AEDs for 6 months. Pre-operative CT scans demonstrating inner subdural membranes may guide one to target the treatment to allow release of this tension band. Mini-craniotomy with careful fenestration of the inner membrane is very effective for this. Brain re-expansion and re-establishment of normal brain interstitial flow may be important in long term outcomes with cSDH and may be related to the recent interests in brain glymphatics and dural lymphatics.
随着人口老龄化加剧和抗凝药物使用增多,慢性硬膜下血肿(cSDH)在全球范围内日益普遍。不同的手术、药物和血管内治疗方法成功率各异。主要的神经外科干预措施包括cSDH钻孔引流术以及有或无内膜开窗的微创开颅术/开颅术。cSDH治疗成败的关键评估指标一直是症状性复发率,历史上该复发率在5%至30%之间。通过CT扫描对硬膜下内膜进行术前预测,以此指导我们决定是否进行微创开颅术。释放内膜有助于大脑扩张,并可能改善类淋巴系统流动。回顾性分析了2018年7月至2020年9月期间,在一家四级学术医疗中心/一级创伤中心由一名神经外科医生连续进行的34例cSDH清除微创开颅术。从电子病历中提取患者特征[年龄、性别、入院时格拉斯哥昏迷评分(GCS)、格拉斯哥预后评分(GOS)、术前CT显示的硬膜下内膜、中线移位(MLS)、cSDH宽度、内膜开窗、cSDH复发、术后癫痫、感染、住院时间]。29例患者将微创开颅术作为cSDH的主要治疗方法。平均年龄为68.9±19.7岁(范围22 - 102岁),术前平均GCS为14.5±1.1,平均MLS为6.75±4.2毫米,cSDH平均最大厚度为17.7±6.0毫米。24例为单侧,5例为双侧,共进行了34次开颅手术。33例患者术前头部CT有内膜征象,除1例开颅手术未显示这些特征性CT表现外,所有病例均对硬膜下内膜进行了开窗。平均手术时间为79.5±26.0分钟。所有患者影像学和临床症状均有改善。MLS平均改善3.85±2.69。在6个月的随访期间,无症状性复发、再次手术、手术部位感染或死亡病例。1例患者术后癫痫发作,使用抗癫痫药物治疗6个月。术前CT扫描显示硬膜下内膜可能有助于指导治疗,以解除这一张力带。为此,仔细对内膜进行开窗的微创开颅术非常有效。大脑再扩张和脑间质正常流动的重建可能对cSDH的长期预后很重要,这可能与近期对脑类淋巴系统和硬脑膜淋巴管的研究兴趣有关。