Ingleby Fiona C, Woods Laura M, Atherton Iain M, Baker Matthew, Elliss-Brookes Lucy, Belot Aurélien
Department of Non-Communicable Disease Epidemiology, Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK.
School of Health & Social Care, Edinburgh Napier University, Edinburgh, UK.
SSM Popul Health. 2021 May 8;14:100815. doi: 10.1016/j.ssmph.2021.100815. eCollection 2021 Jun.
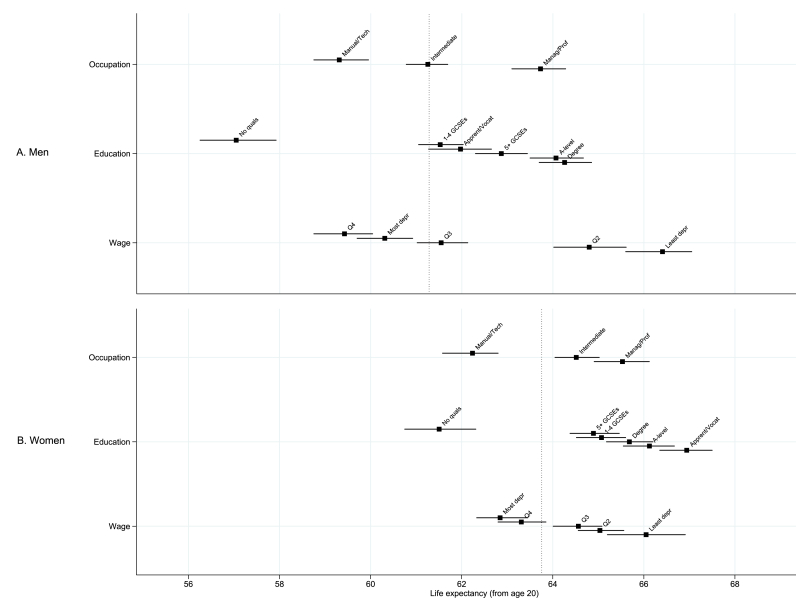
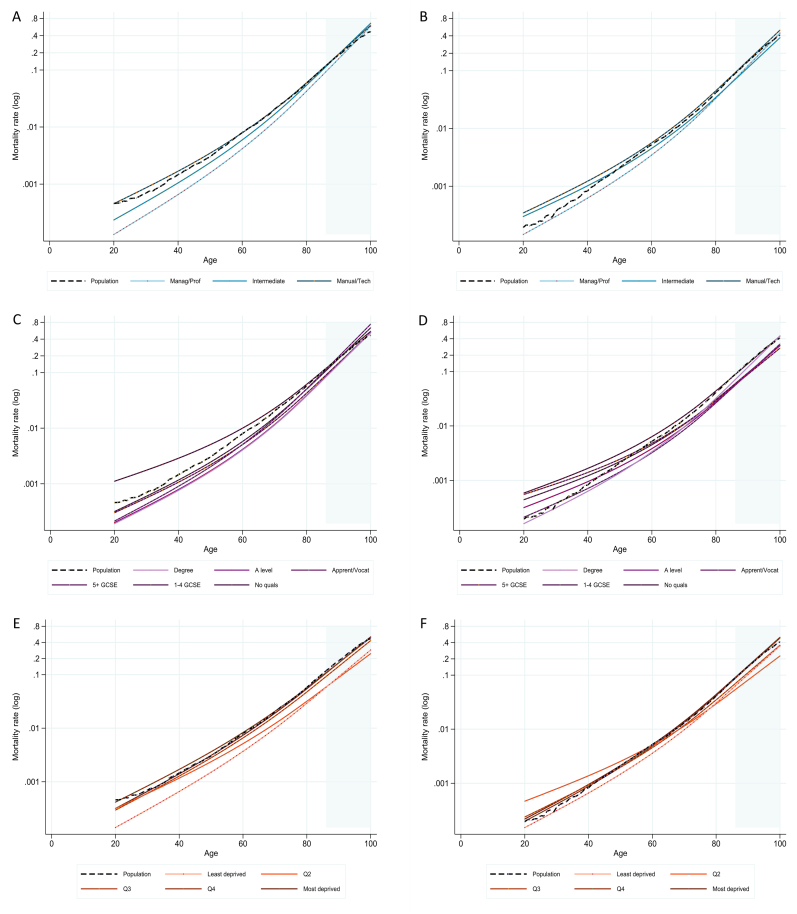
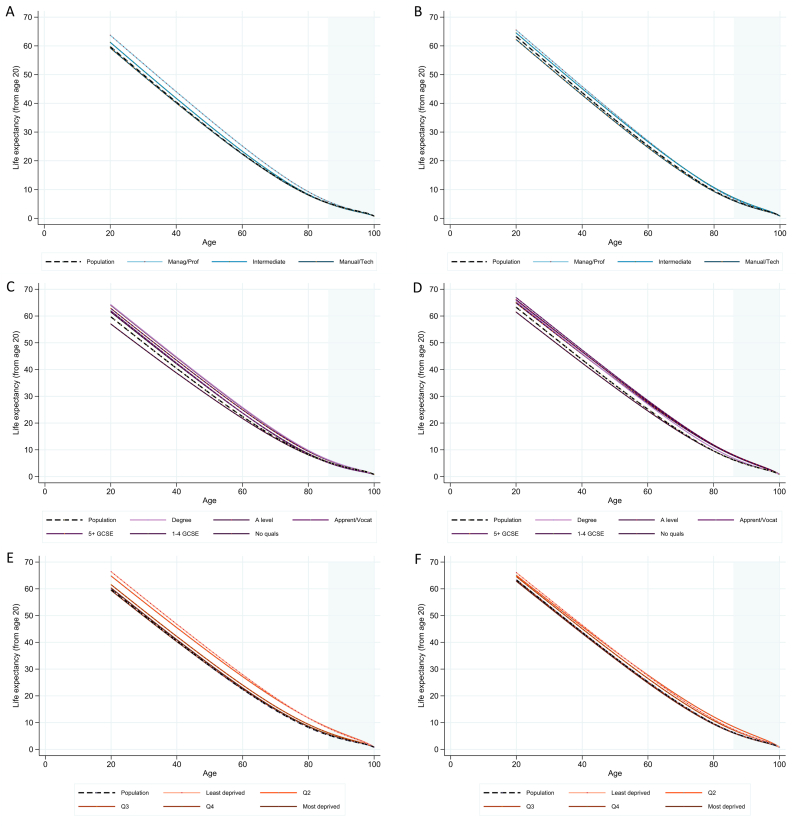
People who live in more deprived areas have poorer health outcomes, and this inequality is a major driver of health and social policy. Many interventions targeting these disparities implicitly assume that poorer health is predominantly associated with area-level factors, and that these inequalities are the same for men and women. However, health differentials due to individual socio-economic status (SES) of men and women are less well documented. We used census data linked to the ONS Longitudinal Study to derive individual-level SES in terms of occupation, education and estimated wage, and examined differences in adult mortality and life expectancy. We modelled age-, sex- and SES-specific mortality using Poisson regression, and summarised mortality differences using life expectancy at age 20. We compared the results to those calculated using area-level deprivation metrics. Wide inequalities in life expectancy between SES groups were observed, although differences across SES groups were smaller for women than for men. The widest inequalities were found across men's education (7.2-year (95% CI: 3.0-10.1) difference in life expectancy between groups) and wage (7.0-year (95% CI: 3.5-9.8) difference), and women's education (5.4-year (95% CI: 2.2-8.1) difference). Men with no qualifications had the lowest life expectancy of all groups. In terms of the number of years' difference in life expectancy, the inequalities measured here with individual-level data were of a similar magnitude to inequalities identified previously using area-level deprivation metrics. These data show that health inequalities are as strongly related to individual SES as to area-level deprivation, highlighting the complementary usefulness of these different metrics. Indeed, poor outcomes are likely to be a product of both community and individual influences. Current policy which bases health spending decisions on evidence of inequalities between geographical areas may overlook individual-level SES inequalities for those living in affluent areas, as well as missing important sex differences.
生活在贫困地区的人群健康状况较差,这种不平等是健康和社会政策的主要推动因素。许多针对这些差异的干预措施隐含地假定,较差的健康状况主要与地区层面的因素相关,并且这些不平等在男性和女性中是相同的。然而,关于男性和女性个体社会经济地位(SES)导致的健康差异,相关记录较少。我们使用与英国国家统计局纵向研究相关联的人口普查数据,从职业、教育和估计工资方面得出个体层面的SES,并研究了成人死亡率和预期寿命的差异。我们使用泊松回归对年龄、性别和SES特定的死亡率进行建模,并使用20岁时的预期寿命总结死亡率差异。我们将结果与使用地区层面贫困指标计算的结果进行了比较。SES组之间的预期寿命存在很大差异,尽管女性SES组之间的差异小于男性。最大的差异出现在男性的教育程度(组间预期寿命相差7.2年(95%置信区间:3.0 - ))和工资(相差7.0年(95%置信区间:3.5 - 9.8))以及女性的教育程度(相差5.4年(95%置信区间:2.2 - 8.1))方面。没有学历的男性预期寿命在所有组中最低。就预期寿命的年数差异而言,这里用个体层面数据衡量的不平等程度与先前使用地区层面贫困指标确定的不平等程度相似。这些数据表明,健康不平等与个体SES的关联程度与地区层面贫困相同,凸显了这些不同指标的互补有用性。事实上,不良结果可能是社区和个体影响共同作用的产物。当前基于地理区域间不平等证据做出健康支出决策的政策,可能会忽视富裕地区居民的个体层面SES不平等,以及重要的性别差异。 10.1))