Cheema Sana G, Hermanns Christina, Coda Reed G, Tarakemeh Armin, Mullen Scott M, Schroeppel John Paul, Vopat Bryan G, Mulcahey Mary K
Department of Orthopaedic Surgery, University of Kansas Health System, Kansas City, Kansas, U.S.A.
Department of Orthopaedic Surgery, Tulane University School of Medicine, New Orleans, Louisiana, U.S.A.
Arthrosc Sports Med Rehabil. 2021 Mar 18;3(2):e427-e433. doi: 10.1016/j.asmr.2020.10.007. eCollection 2021 Apr.
The purpose of this study was to assess the availability and variability of publicly accessible acromioclavicular (AC) joint reconstruction rehabilitation protocols.
Protocols were identified by searching the websites of orthopedic surgery residency programs in the United States located from the Fellowship and Residency Electronic Interactive Database Access System. Private practice groups with publicly available protocols were also included.
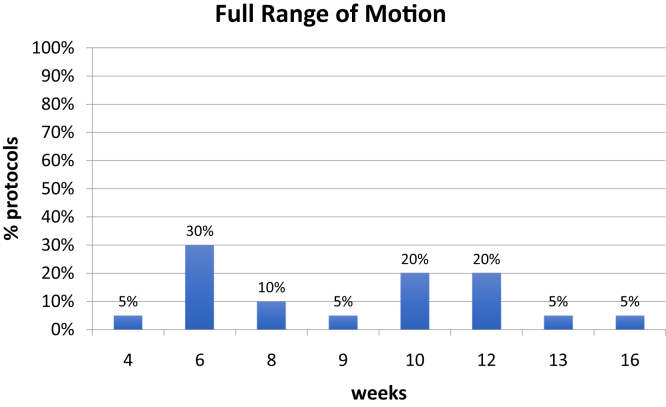
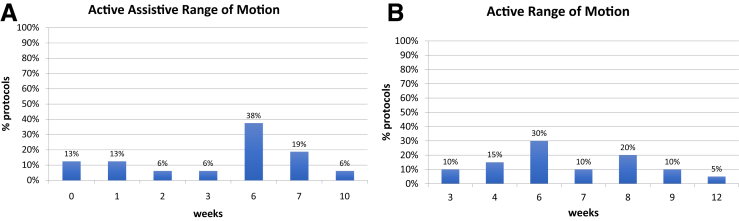
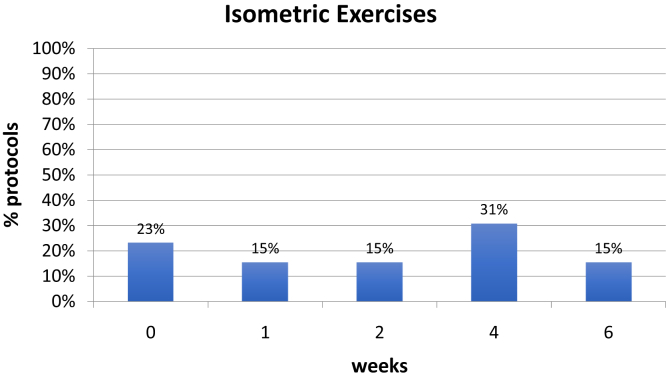
Twenty-one protocols were included for review. Four of 14 (29%) protocols suggested starting passive range of motion (ROM) at postoperative week 2. Six of 20 (30%) protocols recommended initiation of full ROM at 6 weeks. Active ROM beginning at 6 weeks was recommended by 6 of 20 (30%) protocols. Six of 16 (38%) protocols recommended initiating active assisted ROM at 6 weeks. Sling immobilization for 6 weeks was recommended by 8 of 18 (44%) protocols. Shoulder isometric exercise initiated at 4 weeks was recommended by 4 of 13 (31%) protocols. Seven of 21 (33%) protocols recommended initiating shoulder strengthening at 12 weeks postoperatively. Return to sport time was included in 17 (81%) protocols with a range of 12 to 48 weeks (mean, 22 weeks).
There was substantial variability in publicly accessible AC joint rehabilitation protocols, including a wide range in the recommendations for appropriate time to return to sport. Although strengthening exercises, active ROM, and active assisted ROM were recommended by most protocols, there were considerable differences in recommendations for when to initiate these rehabilitation components.
Rehabilitation is important for outcomes of AC joint reconstruction. This study shows the variability present in rehabilitation recommendations among online-accessible AC joint reconstruction rehabilitation protocols.
本研究旨在评估公开可用的肩锁关节(AC)重建康复方案的可用性和变异性。
通过搜索美国骨科手术住院医师培训项目的网站来确定方案,这些网站来自奖学金和住院医师电子交互式数据库访问系统。还纳入了有公开可用方案的私人执业团体。
共纳入21个方案进行审查。14个方案中有4个(29%)建议在术后第2周开始被动活动度(ROM)训练。20个方案中有6个(30%)建议在6周时开始进行全范围ROM训练。20个方案中有6个(30%)建议在6周时开始主动ROM训练。16个方案中有6个(38%)建议在6周时开始主动辅助ROM训练。18个方案中有8个(44%)建议使用吊带固定6周。13个方案中有4个(31%)建议在4周时开始进行肩部等长运动。21个方案中有7个(33%)建议在术后12周开始进行肩部强化训练。17个(81%)方案中包含了恢复运动的时间,范围为12至48周(平均22周)。
公开可用的AC关节康复方案存在很大差异,包括在恢复运动的适当时间建议方面差异很大。尽管大多数方案都推荐进行强化运动、主动ROM训练和主动辅助ROM训练,但在开始这些康复内容的时间建议上存在相当大的差异。
康复对AC关节重建的结果很重要。本研究显示了在线可获取的AC关节重建康复方案中康复建议存在的变异性。