Myriad Genetics, Inc., Salt Lake City, UT.
Cape Cod Healthcare, Mashpee, MA.
JCO Precis Oncol. 2021 Jan 28;5. doi: 10.1200/PO.20.00246. eCollection 2021.
Screening and prevention decisions for women at increased risk of developing breast cancer depend on genetic and clinical factors to estimate risk and select appropriate interventions. Integration of polygenic risk into clinical breast cancer risk estimators can improve discrimination. However, correlated genetic effects must be incorporated carefully to avoid overestimation of risk.
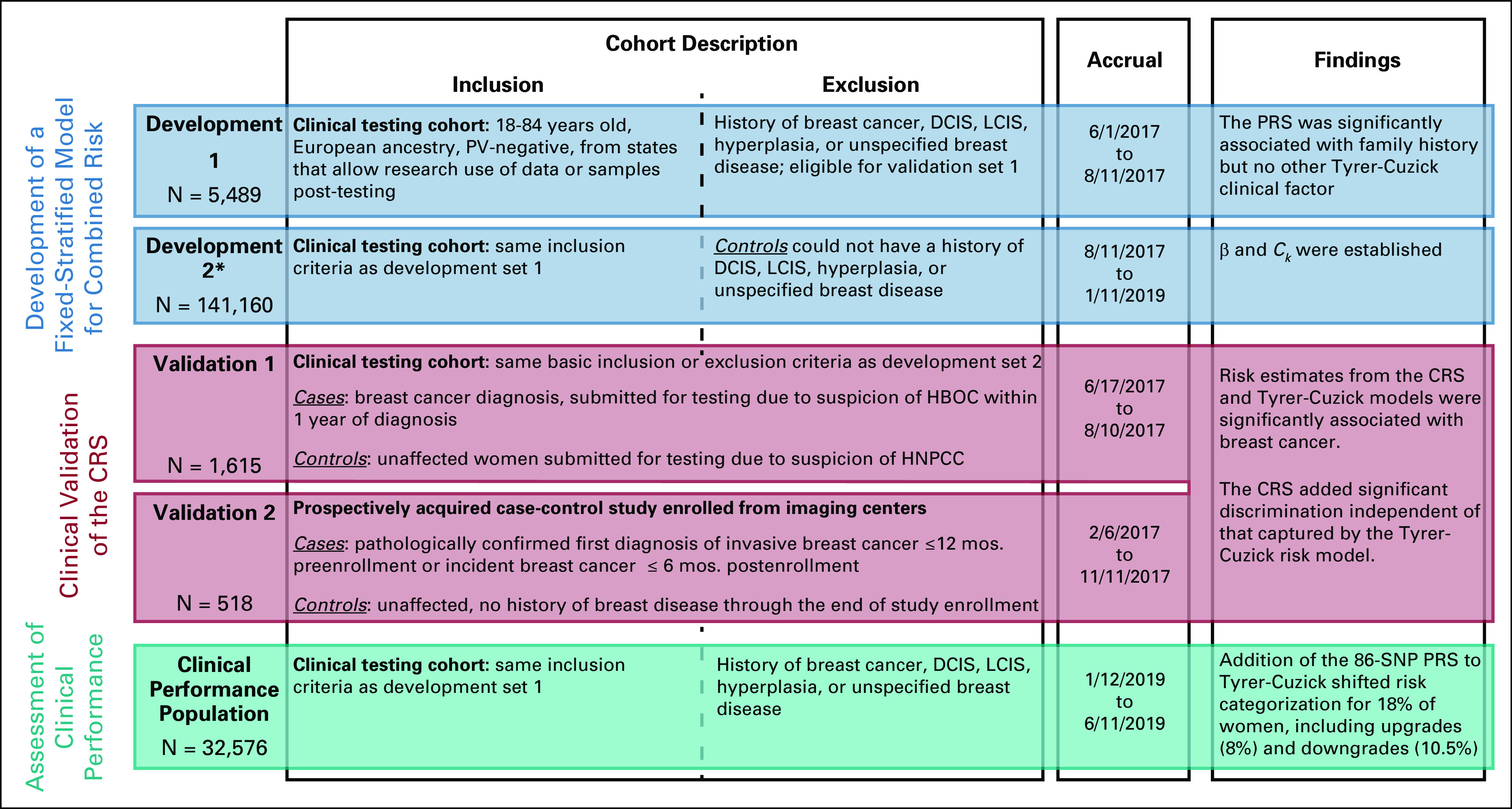
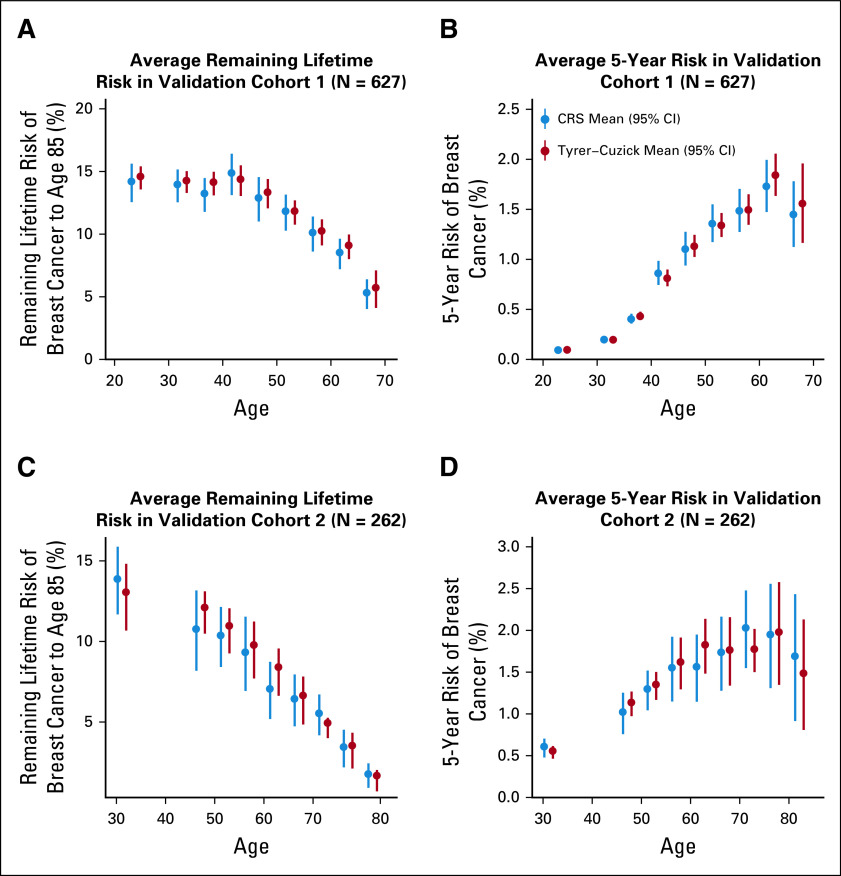
A novel Fixed-Stratified method was developed that accounts for confounding when adding a new factor to an established risk model. A combined risk score (CRS) of an 86-single-nucleotide polymorphism polygenic risk score and the Tyrer-Cuzick v7.02 clinical risk estimator was generated with attenuation for confounding by family history. Calibration and discriminatory accuracy of the CRS were evaluated in two independent validation cohorts of women of European ancestry (N = 1,615 and N = 518). Discrimination for remaining lifetime risk was examined by age-adjusted logistic regression. Risk stratification with a 20% risk threshold was compared between CRS and Tyrer-Cuzick in an independent clinical cohort (N = 32,576).
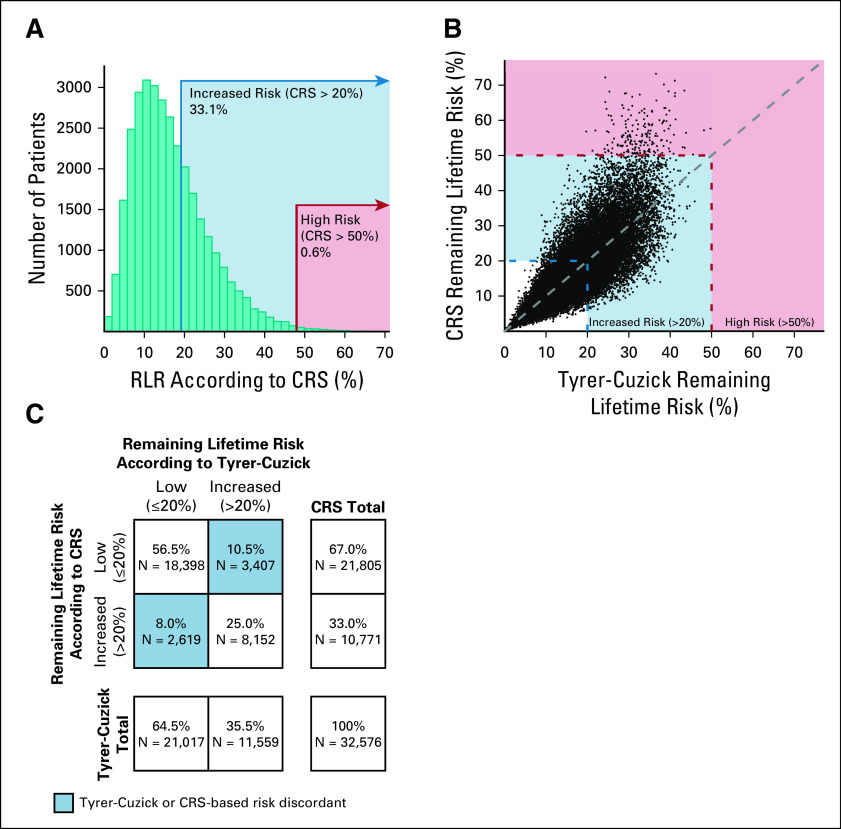
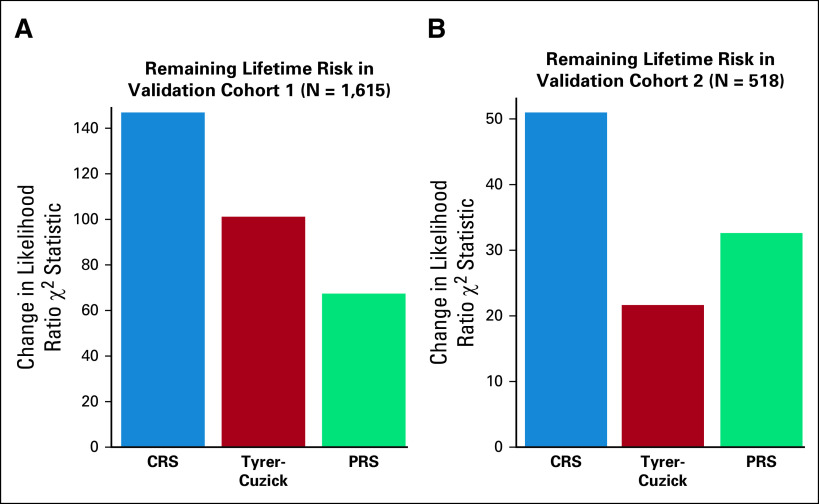
Simulation studies confirmed that the Fixed-Stratified method produced accurate risk estimation across patients with different family history. In both validation studies, CRS and Tyrer-Cuzick were significantly associated with breast cancer. In an analysis with both CRS and Tyrer-Cuzick as predictors of breast cancer, CRS added significant discrimination independent of that captured by Tyrer-Cuzick ( < 10 in validation 1; < 10 in validation 2). In an independent cohort, 18% of women shifted breast cancer risk categories from their Tyrer-Cuzick-based risk compared with risk estimates by CRS.
Integrating clinical and polygenic factors into a risk model offers more effective risk stratification and supports a personalized genomic approach to breast cancer screening and prevention.
对于罹患乳腺癌风险较高的女性,其筛查和预防决策取决于遗传和临床因素,以评估风险并选择合适的干预措施。将多基因风险纳入临床乳腺癌风险评估器可以提高区分度。然而,为了避免风险的高估,必须谨慎地整合相关的遗传效应。
开发了一种新的固定分层方法,用于在既定风险模型中添加新因素时考虑混杂因素。通过对家族史进行混杂因素衰减,生成了一个包含 86 个单核苷酸多态性多基因风险评分和 Tyrer-Cuzick v7.02 临床风险评估器的综合风险评分(CRS)。在两个独立的欧洲裔女性验证队列(N=1615 和 N=518)中,评估了 CRS 的校准和判别准确性。通过年龄调整的逻辑回归,评估了剩余终生风险的判别能力。在一个独立的临床队列(N=32576)中,将 CRS 和 Tyrer-Cuzick 的 20%风险阈值风险分层进行了比较。
模拟研究证实,固定分层方法在不同家族史的患者中都能准确地进行风险估计。在两个验证研究中,CRS 和 Tyrer-Cuzick 均与乳腺癌显著相关。在一项将 CRS 和 Tyrer-Cuzick 作为乳腺癌预测因子的分析中,CRS 增加了独立于 Tyrer-Cuzick 捕捉到的显著判别力(验证 1<10;验证 2<10)。在一个独立的队列中,与 Tyrer-Cuzick 相比,有 18%的女性的乳腺癌风险类别发生了变化,而这是由 CRS 估计的。
将临床和多基因因素整合到风险模型中可以提供更有效的风险分层,并支持个性化的基因组方法来进行乳腺癌筛查和预防。