Department of Plastic and Cosmetic Surgery, Xinqiao Hospital, Army Medical University, Chongqing, People's Republic of China.
Department of Cardiovascular Surgery, Xinqiao Hospital, Army Medical University, Chongqing, People's Republic of China.
Int Wound J. 2022 Feb;19(2):253-261. doi: 10.1111/iwj.13626. Epub 2021 May 25.
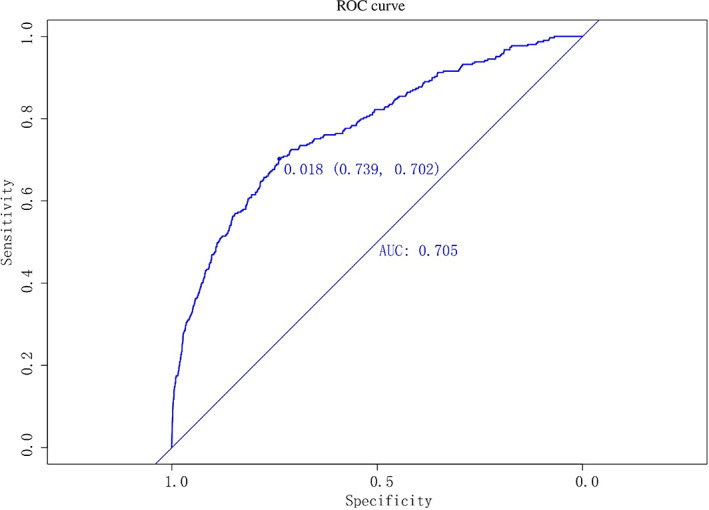
Presently, the incidence and mortality rates of sternal incision problems (SIPs) after thoracotomy remain high, and no effective preventive measures are available. The data on 23 182 patients at Xinqiao Hospital, Army Medical University treated with median sternotomy from 1 August 2009 to 31 July 2019 were retrospectively reviewed. A prediction model of SIPs after median thoracotomy was established using R software and then validated using the bootstrap method. Next, the validity and accuracy of the model were tested and evaluated. In total, 15 426 cases met the requirements of the present study, among which 309 cases were diagnosed with SIPs, with an incidence rate of 2%. The body mass index (BMI), intensive care unit (ICU) time, diabetes mellitus, and revision for bleeding were identified as independent risk factors for postoperative SIPs. The nomogram model achieved good discrimination (73.9%) and accuracy (70.2%) in predicting the risk of SIPs after median thoracotomy. Receiver operating characteristic curve analysis showed that the area under curve of the model was 0.705 (95% confidence interval [CI]: 0.746-0.803); the Hosmer-Lemeshow test showed that χ = 6.987 and P = 0.538, and the fitting degree of the calibration curve was good. Additionally, the clinical decision curve showed that the net benefit of the model was greater than 0, and the clinical application value was high. The nomogram based on BMI, ICU time, diabetes mellitus, and revision for bleeding can predict the individualised risk of SIPs after median sternotomy, showing good discrimination and accuracy, and has high clinical application value. It also provides significant guidance for screening high-risk populations and developing intervention strategies.
目前,剖胸术后胸骨切口问题(SIP)的发病率和死亡率仍然很高,且尚无有效的预防措施。回顾性分析 2009 年 8 月 1 日至 2019 年 7 月 31 日陆军军医大学新桥医院行正中开胸术的 23182 例患者的资料。使用 R 软件建立了正中开胸术后 SIP 的预测模型,然后使用自举法进行验证。接下来,测试并评估了模型的有效性和准确性。共纳入 15426 例符合本研究要求的患者,其中 309 例诊断为 SIP,发病率为 2%。体重指数(BMI)、重症监护病房(ICU)时间、糖尿病和因出血而修订术式被确定为术后 SIP 的独立危险因素。列线图模型在预测正中开胸术后 SIP 风险方面具有良好的区分度(73.9%)和准确性(70.2%)。受试者工作特征曲线分析显示,模型的曲线下面积为 0.705(95%置信区间[CI]:0.746-0.803);Hosmer-Lemeshow 检验显示 χ2=6.987,P=0.538,校准曲线拟合度良好。此外,临床决策曲线显示,模型的净效益大于 0,具有较高的临床应用价值。基于 BMI、ICU 时间、糖尿病和修订术式的列线图可以预测正中开胸术后 SIP 的个体风险,具有良好的区分度和准确性,具有较高的临床应用价值。它还为筛选高危人群和制定干预策略提供了重要指导。