Department of Cardiology, Sørlandet Hospital, Arendal, Box 783, Stoa, 4809 Arendal, Norway.
Oslo Centre of Biostatistics and Epidemiology, Oslo University Hospital, Oslo, Norway.
Eur Heart J Cardiovasc Pharmacother. 2022 Aug 11;8(5):442-451. doi: 10.1093/ehjcvp/pvab041.
Primary percutaneous coronary intervention (pPCI) is the preferred reperfusion strategy in patients with ST-segment elevation myocardial infarction (STEMI) provided it can be performed within 120 min from diagnosis. However, it is unclear whether pPCI or a pharmaco-invasive (P-I) strategy is the best choice in patients who cannot receive timely pPCI. The aim of the present study was to compare outcomes after delayed and late pPCI vs. a P-I strategy in STEMI patients who did not receive timely pPCI.
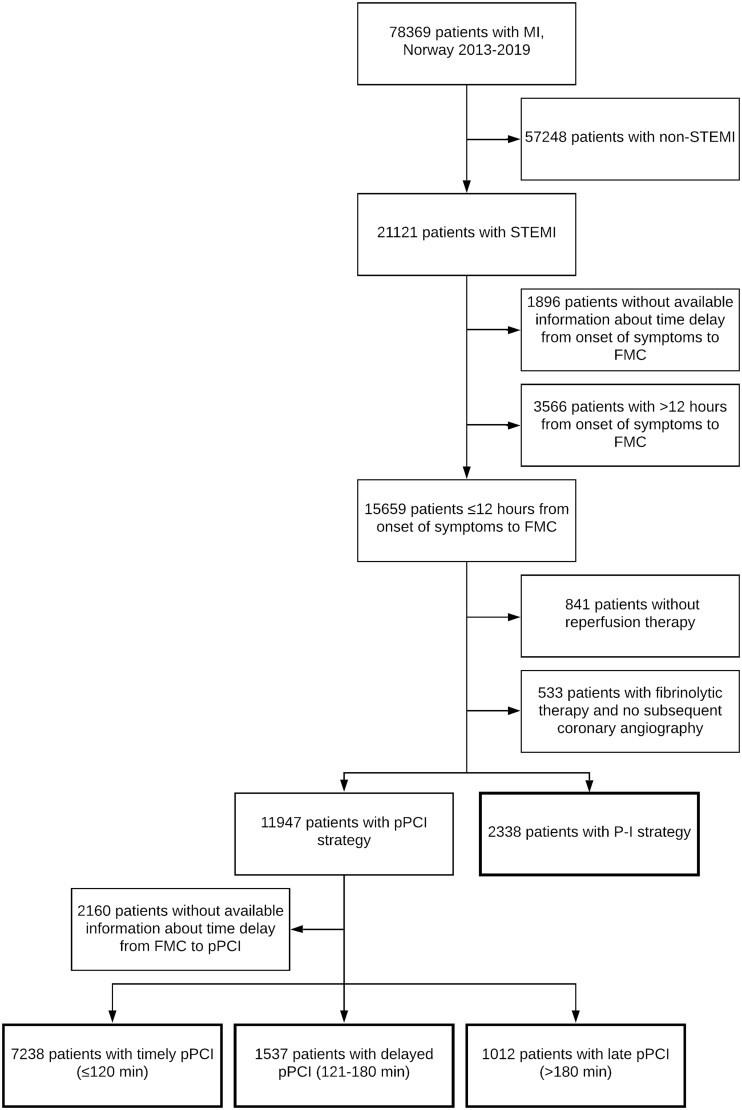
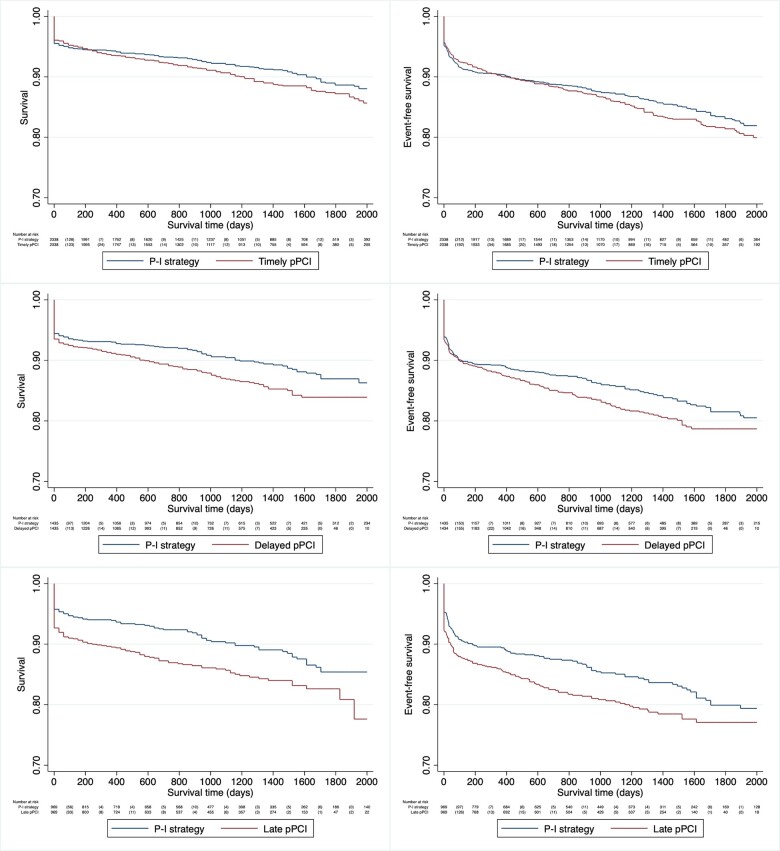
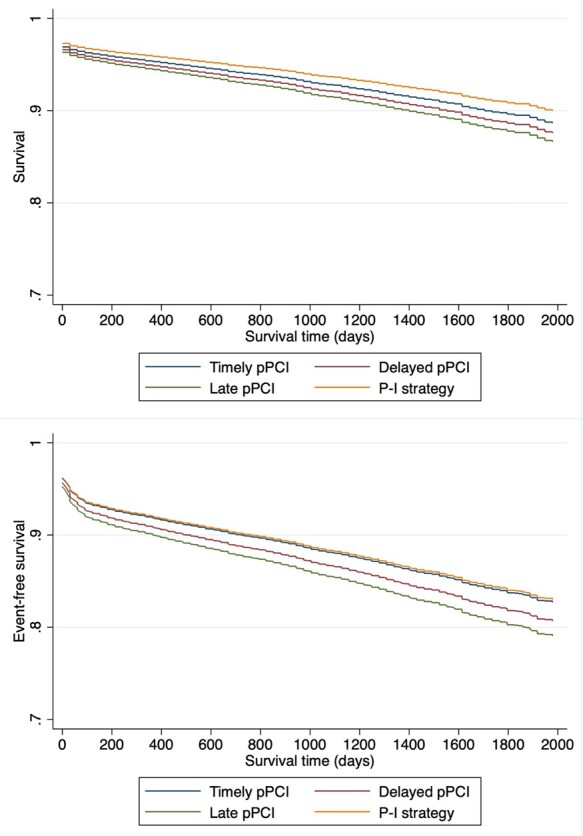
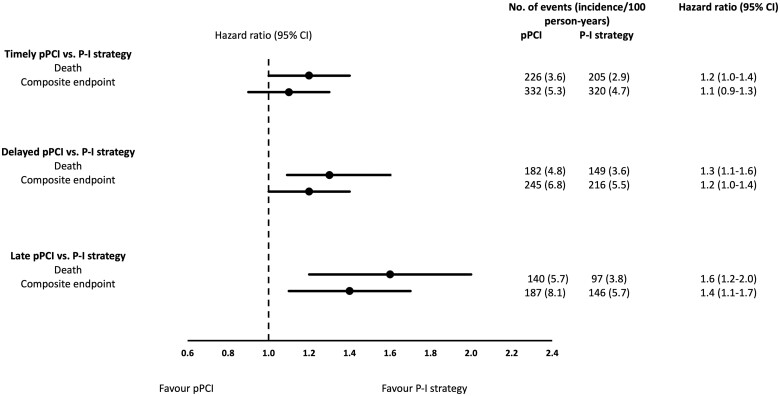
All patients with STEMI registered in the Norwegian Myocardial Infarction Registry (NORMI) between 2013 and 2019, with ≤12 h from symptom onset to first medical contact and available timelines were included in the study. The primary outcome was all-cause mortality, and follow-up was through 2019. A total of 21 121 (27% of 78 368) STEMI patients were registered in the NORMI. Among patients who met the inclusion criteria, 7238 (54%) patients underwent timely pPCI, 1537 (11%) delayed pPCI (121-180 min), 1012 (7%) late pPCI (>180 min), and 2338 (17%) patients were treated with a P-I strategy. After a median follow-up time of 2.5 years, mortality was higher in the delayed pPCI [adjusted hazard ratio (HR) 1.3, 95% confidence interval (CI) 1.0-1.5] and in the late pPCI group (adjusted HR 1.4, 95% CI 1.1-1.7) compared to the P-I strategy group, but bleeding complications were more frequent after P-I strategy.
In STEMI patients who did not receive timely percutaneous coronary intervention, a P-I strategy seemed to be associated with better long-term survival compared to delayed/late pPCI.
在 ST 段抬高型心肌梗死(STEMI)患者中,直接经皮冠状动脉介入治疗(pPCI)是首选的再灌注策略,前提是能够在诊断后 120 分钟内进行。然而,对于无法及时接受 pPCI 的患者,pPCI 与药物介入(P-I)策略哪一种是最佳选择尚不清楚。本研究旨在比较未能及时接受 pPCI 的 STEMI 患者延迟和晚期 pPCI 与 P-I 策略治疗后的结局。
本研究纳入了 2013 年至 2019 年期间在挪威心肌梗死登记处(NORMI)登记的所有 STEMI 患者,其从症状发作到首次医疗接触的时间≤12 小时,且时间线可用。主要结局为全因死亡率,随访至 2019 年。共登记了 21121 例(78368 例的 27%)STEMI 患者。在符合纳入标准的患者中,7238 例(54%)患者接受了及时的 pPCI,1537 例(11%)接受了延迟的 pPCI(121-180 分钟),1012 例(7%)接受了晚期 pPCI(>180 分钟),2338 例(17%)患者接受了 P-I 策略。中位随访时间为 2.5 年后,与 P-I 策略组相比,延迟 pPCI 组(校正后的危险比 [HR] 1.3,95%置信区间 [CI] 1.0-1.5)和晚期 pPCI 组(校正后的 HR 1.4,95% CI 1.1-1.7)的死亡率更高,但 P-I 策略后出血并发症更常见。
在未能及时接受经皮冠状动脉介入治疗的 STEMI 患者中,与延迟/晚期 pPCI 相比,P-I 策略似乎与长期生存改善相关。