Chiarotto James A, Dranitsaris George
Department of Medicine, The Scarborough Health Network, Toronto, Ontario, Canada.
Augmentium Pharma Consulting, Inc., Toronto, Ontario, Canada.
Cancer Manag Res. 2021 May 19;13:4087-4094. doi: 10.2147/CMAR.S307713. eCollection 2021.
To look at how the absolute neutrophil count (ANC) is used by community oncologists as the main factor in ordering adjuvant mFOLFOX6 for colorectal cancer. This study reports on how this decision impacts chemotherapy delays, effects received dose intensity (RDI), and increases the use of granulocyte-colony-stimulating factor (G-CSF).
A retrospective chart review was conducted for all patients receiving adjuvant mFOLFOX6 for colorectal cancer at a two-site community hospital in Toronto, Ontario, Canada, between July 2013 and March 2019. Seven physicians treated 140 patients, who made 1636 clinic visits to receive 1461 cycles of prescribed chemotherapy.
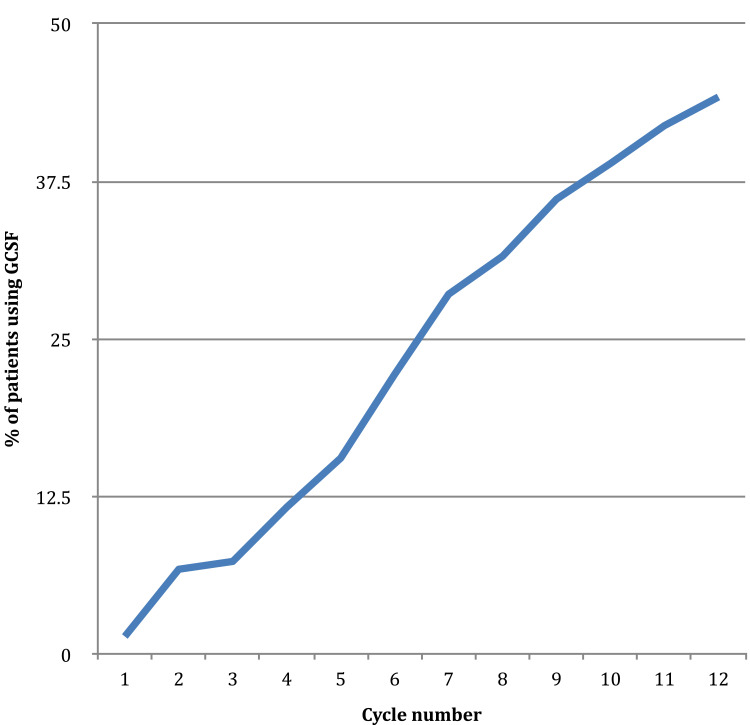
The mean ANC per physician associated with a decision to give chemotherapy ranged from 1.05×10/L (95% CI 0.98-1.13×10/L) to 1.5x10/L with a decision to delay if the ANC was lower. Subsequent cycles were then supported by G-CSF with very similar ANC decision levels for dose delay. Physicians were more likely to prescribe chemotherapy with higher pretreatment ANC, r=0.3 (p<0.000). G-CSF was used in 24.6% of cycles and usage had grown to 44.2% by the 12th cycle; physician use ranged from 0.36% to 54.2% of cycles. Secondary prophylaxis was the indication in 94.7% of cases. There was an inverse relationship between the frequency of G-CSF use and the RDI of continuous infusion 5FU, r=-0.26 (p<0.001). There were delays for 8.8% of visits for cycles not supported by G-CSF and, surprisingly, 15.9% of visits for cycles supported by G-CSF. Neutropenia caused 61.6% of delays for chemotherapy cycles not supported by G-CSF and 44.1% for cycles supported by G-CSF.
Physicians required a pretreatment ANC of 1.05-1.5×10/L before prescribing mFOLFOX6 chemotherapy. When ANC was low, a dose delay and secondary prophylaxis with G-CSF failed to consistently achieve the much sought after ANC. This then caused more delay, reduced RDI and increased expense for both patients and the system. Fewer delays, less G-CSF and increased RDI would have resulted with reduced reliance on ANC and adoption of chemotherapy dose reduction.
研究社区肿瘤学家如何将绝对中性粒细胞计数(ANC)作为决定为结直肠癌患者开具辅助性mFOLFOX6化疗方案的主要因素。本研究报告了这一决定如何影响化疗延迟、实际接受剂量强度(RDI)以及增加粒细胞集落刺激因子(G-CSF)的使用。
对2013年7月至2019年3月期间在加拿大安大略省多伦多市一家有两个院区的社区医院接受辅助性mFOLFOX6治疗的所有结直肠癌患者进行回顾性病历审查。7名医生治疗了140例患者,这些患者进行了1636次门诊就诊,接受了1461个周期的规定化疗。
每位医生决定进行化疗时的平均ANC范围为1.05×10⁹/L(95%CI 0.98 - 1.13×10⁹/L)至1.5×10⁹/L,若ANC较低则决定延迟化疗。随后的周期通过G-CSF支持,剂量延迟的ANC决定水平非常相似。医生更倾向于在预处理ANC较高时开具化疗处方,r = 0.3(p < 0.000)。24.6%的化疗周期使用了G-CSF,到第12个周期时使用率已增至44.2%;医生的使用比例从0.36%到54.2%不等。94.7%的病例使用G-CSF的指征为二级预防。G-CSF使用频率与持续输注5-氟尿嘧啶的RDI呈负相关,r = -0.26(p < 0.001)。在未使用G-CSF支持的化疗周期中,8.8%的门诊就诊出现延迟,令人惊讶的是,在使用G-CSF支持的化疗周期中,15.9%的门诊就诊出现延迟。中性粒细胞减少导致未使用G-CSF支持的化疗周期中61.6%出现延迟,使用G-CSF支持的化疗周期中44.1%出现延迟。
医生在开具mFOLFOX6化疗处方前要求预处理ANC为1.05 - 1.5×10⁹/L。当ANC较低时,剂量延迟和使用G-CSF进行二级预防未能始终如一地达到人们所追求的ANC水平。这进而导致更多延迟、降低了RDI,并增加了患者和医疗系统的费用。减少对ANC的依赖并采用化疗剂量降低措施,本可减少延迟、减少G-CSF的使用并提高RDI。