Riga Stradins University, 16 Dzirciema Street, Riga, LV-1007, Latvia.
Centre of Cardiac Surgery, Pauls Stradins Clinical University Hospital, 13 Pilsonu Street, Riga, LV-1002, Latvia.
J Cardiothorac Surg. 2021 May 27;16(1):147. doi: 10.1186/s13019-021-01532-9.
Up to 30% or even more of all infective endocarditis (IE) cases are recognized as blood culture negative, meaning that the causative agent is left unidentified. The prompt diagnosis together with the identification of causative microorganism and targeted antibiotic treatment can significantly impact the prognosis of the disease and further patient's health status. In some studies, blood culture negative endocarditis has been shown to be associated with delayed diagnosis, worse outcome and course of the disease, and a greater number of intra and postoperative complications.
We retrospectively analysed the medical records of all patients who underwent cardiac surgery for endocarditis between years 2016 and 2019. The aim of this study was to analyse short and long-term mortality and differences of laboratory, clinical and echocardiography parameters in patients with blood culture positive endocarditis (BCPE) and blood culture negative endocarditis (BCNE) and its possible impact on the clinical outcome.
In our study population were 114 (55.1%) blood culture positive and 93 (44.9%) blood culture negative cases of infectious endocarditis. The most common pathogens in the blood culture positive IE group were S.aureus in 36 cases (31.6%), Streptococcus spp. in 27 (23.7%), E.faecalis in 24 (21.1%), and other microorganisms in 27 (23.7%). Embolic events were seen in 60 patients (28.9%). In univariate analyses, detection of microorganism, elevated levels of procalcitonin were found to be significantly associated with intrahospital death, however it did not reach statistical significance in multivariate analyses. Among microorganisms, S.aureus was significantly associated with intrahospital death in both univariate and multivariate analyses.
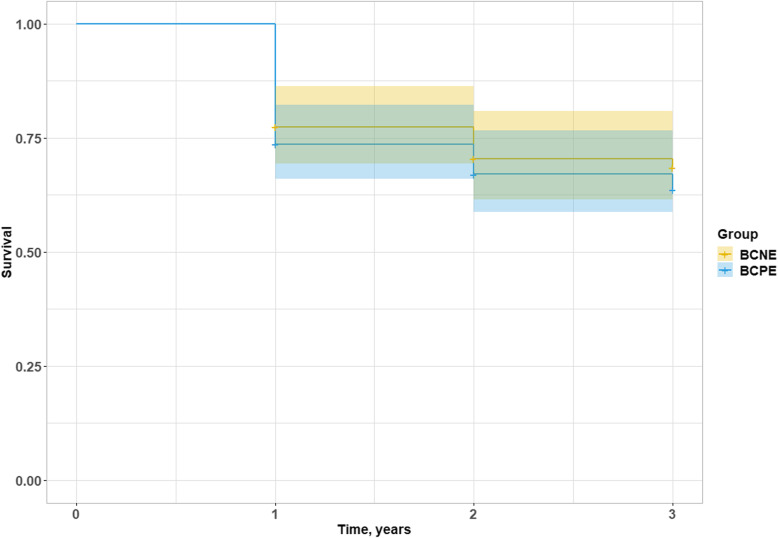
There are no statistically significant differences between groups of BCPE and BCNE in terms of intrahospital mortality, hospital and ICU stay or 3-year mortality. There were higher levels of procalcitonin in BCPE group, however procalcitonin failed to show independent association with mortality in multivariate analysis. The most common microorganism in the BCPE group was S.aureus. It was associated with independently higher intrahospital mortality when compared to other causative microorganisms.
多达 30%甚至更多的感染性心内膜炎(IE)病例被认为是血培养阴性,这意味着致病病原体未被识别。及时诊断以及确定致病微生物并进行靶向抗生素治疗可以显著影响疾病的预后和进一步的患者健康状况。在一些研究中,血培养阴性心内膜炎与诊断延迟、预后和疾病病程较差以及更多的围手术期并发症相关。
我们回顾性分析了 2016 年至 2019 年间接受心脏手术治疗的心内膜炎患者的病历。本研究的目的是分析血培养阳性心内膜炎(BCPE)和血培养阴性心内膜炎(BCNE)患者的短期和长期死亡率以及实验室、临床和超声心动图参数的差异,并分析其对临床结果的可能影响。
在我们的研究人群中,114 例(55.1%)为血培养阳性 IE 病例,93 例(44.9%)为血培养阴性 IE 病例。BCPE 组中最常见的病原体是金黄色葡萄球菌 36 例(31.6%)、链球菌属 27 例(23.7%)、粪肠球菌 24 例(21.1%)和其他微生物 27 例(23.7%)。60 例患者(28.9%)发生栓塞事件。在单因素分析中,检测到微生物和降钙素原水平升高与院内死亡显著相关,但在多因素分析中未达到统计学意义。在微生物中,金黄色葡萄球菌在单因素和多因素分析中均与院内死亡显著相关。
BCPE 和 BCNE 组在院内死亡率、住院时间和 ICU 住院时间或 3 年死亡率方面无统计学差异。BCPE 组降钙素原水平较高,但在多因素分析中降钙素原未能显示与死亡率的独立相关性。BCPE 组最常见的微生物是金黄色葡萄球菌,与其他致病微生物相比,它与院内死亡率独立升高相关。