Sarkar Mihir, Roychowdhoury Satyabrata, Bhakta Subhajit, Raut Sumantra, Nandi Mousumi
Department of Pediatrics, Calcutta Medical College, Kolkata, West Bengal, India.
Indian J Crit Care Med. 2021 Apr;25(4):435-440. doi: 10.5005/jp-journals-10071-23791.
With the advancement of pediatric critical care services across India, many children require prolonged mechanical ventilation (MV), and tracheostomy is recommended to them. However, many pediatric intensivists have concerns regarding the safety, feasibility, and outcome of tracheostomy.We aimed to analyze clinical characteristics, indication, duration, and outcome of tracheostomized children with respect to timing of tracheostomy.
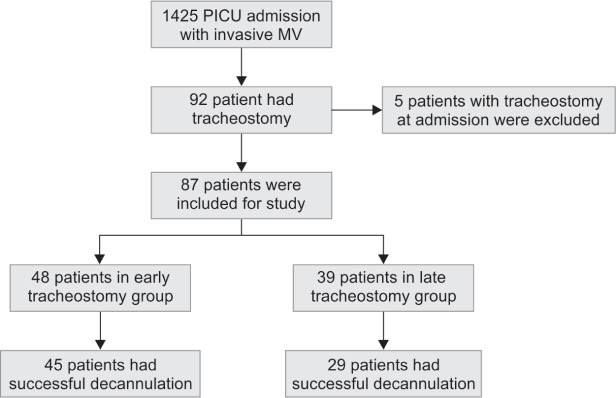
We conducted a retrospective study from the hospital clinical database of consecutive patients below 12 years who had undergone tracheostomy after admission into the pediatric intensive care unit (PICU) for prolonged ventilation (≥96 hours) from January 2015 to December 2019. The study was approved by the Institutional Ethics Committee. Patients were divided into two groups: tracheostomies done within 14 days of MV (early tracheostomy) and patients with tracheostomies performed after 14 days (late tracheostomy). Patients' age, sex, indications, complications, decannulation rate, length of MV, PICU, and hospital stay were analyzed.
Of the 1,425 patients on invasive MV, 87 (6.1%) patients required tracheostomy after a mean 13.37 days of MV. The most common indication was encephalopathy 32 (36.7%) followed by acute respiratory distress syndrome 20 (22.9%). Factors like higher pediatric logistic organ dysfunction score, vasoactive inotrop score, incidence of pretracheostomy ventilator-associated pneumonia, and difficulty in obtaining parental consent were associated with late tracheostomy. The early tracheostomy group had a higher decannulation rate (odds ratio, 5.17; , 0.01) and weaning rate (odds ratio, 5.94; , 0.032). The late tracheostomy group needed a longer duration of MV, PICU, and hospital stay. Complications of tracheostomy were less in the early tracheostomy patients (odds ratio, 2.95; , 0.03).
Early tracheostomy was associated with lower complications, higher successful weaning rates, and less utilization of intensive care facilities in patients receiving prolonged MV.
In the context of scarcity of data on the timing of tracheostomy in children with prolonged ventilation (≥96 hours) the study shows that early (<14 days) tracheostomy is associated with a better outcome.
Sarkar M, Roychowdhoury S, Bhakta S, Raut S, Nandi M. Tracheostomy before 14 Days: Is It Associated with Better Outcomes in Pediatric Patients on Prolonged Mechanical Ventilation? Indian J Crit Care Med 2021;25(4):435-440.
随着印度儿科重症监护服务的发展,许多儿童需要长时间机械通气(MV),并建议对他们进行气管切开术。然而,许多儿科重症监护医生对气管切开术的安全性、可行性和结果存在担忧。我们旨在分析气管切开儿童的临床特征、适应症、持续时间和结果与气管切开时机的关系。
我们对2015年1月至2019年12月期间入住儿科重症监护病房(PICU)进行长时间通气(≥96小时)后接受气管切开术的12岁以下连续患者的医院临床数据库进行了回顾性研究。该研究得到了机构伦理委员会的批准。患者分为两组:MV后14天内进行气管切开术(早期气管切开术)和14天后进行气管切开术的患者(晚期气管切开术)。分析了患者的年龄、性别、适应症、并发症、拔管率、MV持续时间、PICU和住院时间。
在1425例接受有创MV的患者中,87例(6.1%)患者在平均MV 13.37天后需要气管切开术。最常见的适应症是脑病32例(36.7%),其次是急性呼吸窘迫综合征20例(22.9%)。较高的儿科逻辑器官功能障碍评分、血管活性药物评分、气管切开术前呼吸机相关性肺炎的发生率以及获得家长同意困难等因素与晚期气管切开术相关。早期气管切开术组的拔管率较高(优势比,5.17;P<0.01)和撤机率较高(优势比,5.94;P<0.032)。晚期气管切开术组需要更长的MV持续时间、PICU和住院时间。早期气管切开术患者的气管切开术并发症较少(优势比,2.95;P<0.03)。
早期气管切开术与接受长时间MV的患者并发症较低、成功撤机率较高以及重症监护设施利用率较低相关。
在长时间通气(≥96小时)儿童气管切开术时机的数据稀缺的背景下,该研究表明早期(<14天)气管切开术与更好的结果相关。
Sarkar M, Roychowdhoury S, Bhakta S, Raut S, Nandi M. 14天前气管切开术:是否与长时间机械通气的儿科患者更好的结果相关?《印度重症医学杂志》2021;25(4):435 - 440。