Zhu Hong-Min, Zhang Si-Min, Yao Cong, Luo Meng-Qing, Ma Hui-Jing, Lei Tao, Yuan Chun-Hui, Wu Ge-Fei, Hu Jia-Sheng, Cai Chun-Quan, Liu Zhi-Sheng
Pediatric Clinical College of Tianjin Medical University, Tianjin, China.
Department of Neurology, Wuhan Children's Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Front Pediatr. 2021 May 11;9:655074. doi: 10.3389/fped.2021.655074. eCollection 2021.
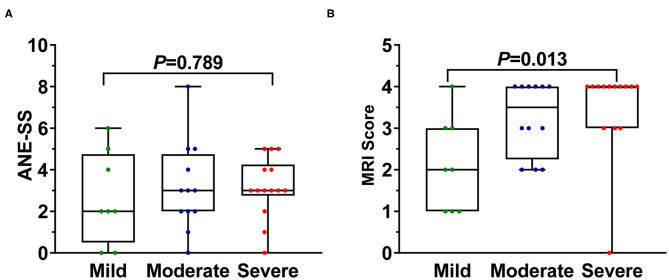
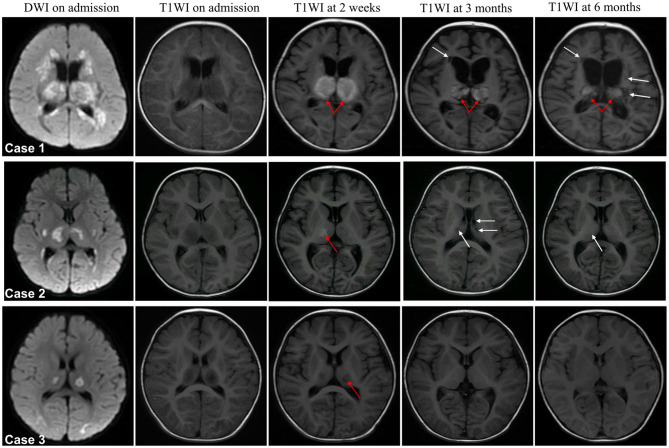
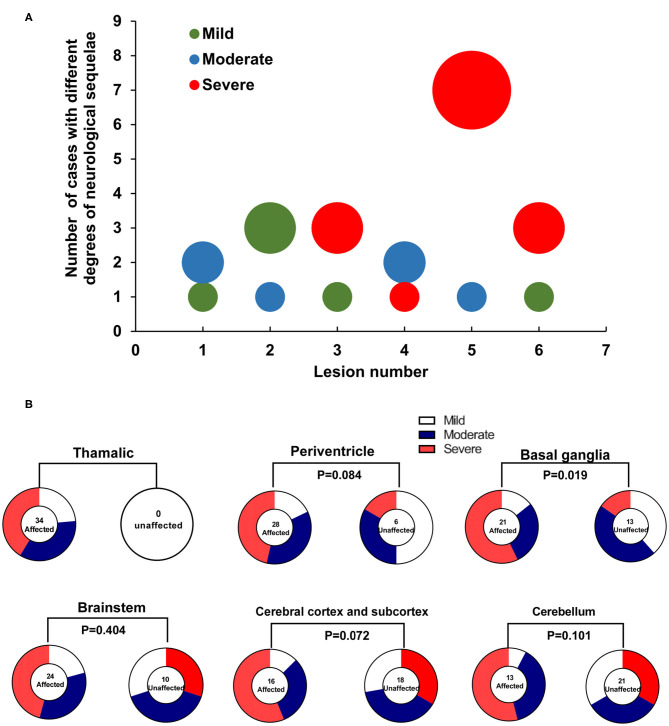
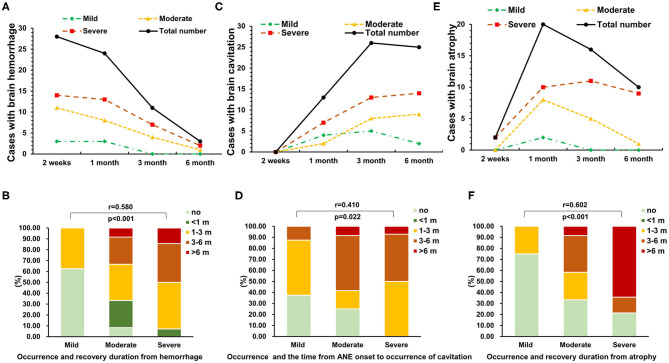
Acute necrotizing encephalopathy of childhood (ANE) is a rare but rapidly progressing encephalopathy. Importantly, the exact pathogenesis and evidence-based treatment is scarce. Thus, we aimed to identify the clinical, imaging, and therapeutic characteristics that associated with prognosis of pediatric ANE patients. A retrospective study was conducted on pediatric patients with ANE who were admitted to Wuhan Children's Hospital between January 2014 and September 2019. All cases met the diagnostic criteria for ANE proposed by Mizuguchi in 1997. The clinical information and follow-up data were collected. The prognostic factors were analyzed by trend chi-square test and Goodman-Kruskal gamma test. A total of 41 ANE patients ranging in age from 8.9 to 142 months were included in this study. Seven cases (17%) died, and the other 34 survivors had different degrees of neurological sequelae. Factors tested to be significantly correlated with the severity of neurological sequelae were the intervals from prodromal infection to acute encephalopathy (G = -0.553), conscious disturbance ( = 0.58), endotracheal intubation ( = 0.423), elevation of alanine aminotransferase ( = 0.345), aspartate aminotransferase ( = 0.393), and cerebrospinal fluid protein ( = 0.490). In addition, dynamic magnetic resonance imaging (MRI) evaluation on follow-up revealed that the total numbers of brain lesion location (χ = 6.29, < 0.05), hemorrhage ( = 0.580), cavitation ( = 0.410), and atrophy ( = 0.602) status were significantly correlated with the severity of neurological sequelae, while early steroid therapy ( = -0.127 and 0.212, respectively) and intravenous immunoglobulin (IVIG) ( = 0.111 and -0.023, respectively) within 24 h or within 72 h after onset showed no association. Intervals from prodromal infection to acute encephalopathy (≤1 day), total numbers of brain lesion location (≥3), the recovery duration of hemorrhage and atrophy (>3 months), and the presence of cavitation predict severe neurological sequelae in pediatric patients with ANE. Early treatments, including steroid therapy and IVIG, had no correlation with better outcomes. Further studies are needed to establish a consensus guideline for the management of ANE.
儿童急性坏死性脑病(ANE)是一种罕见但进展迅速的脑病。重要的是,其确切发病机制和循证治疗方法稀缺。因此,我们旨在确定与小儿ANE患者预后相关的临床、影像学和治疗特征。对2014年1月至2019年9月期间入住武汉儿童医院的小儿ANE患者进行了一项回顾性研究。所有病例均符合水口1997年提出的ANE诊断标准。收集了临床信息和随访数据。通过趋势卡方检验和古德曼-克鲁斯卡尔伽马检验分析预后因素。本研究共纳入41例年龄在8.9至142个月之间的ANE患者。7例(17%)死亡,其他34例幸存者有不同程度的神经后遗症。经检验与神经后遗症严重程度显著相关的因素有前驱感染至急性脑病的间隔时间(G = -0.553)、意识障碍( = 0.58)、气管插管( = 0.423)、丙氨酸转氨酶升高( = 0.345)、天冬氨酸转氨酶升高( = 0.393)和脑脊液蛋白升高( = 0.490)。此外,随访时的动态磁共振成像(MRI)评估显示,脑病变部位总数(χ = 6.29, < 0.05)、出血( = 0.580)、空洞形成( = 0.410)和萎缩( = 0.602)状态与神经后遗症严重程度显著相关,而发病后24小时内或72小时内早期使用类固醇治疗(分别为 = -0.127和0.212)及静脉注射免疫球蛋白(IVIG)(分别为 = 0.111和 -0.023)未显示出相关性。前驱感染至急性脑病的间隔时间(≤1天)、脑病变部位总数(≥3个)、出血和萎缩的恢复持续时间(>3个月)以及空洞形成提示小儿ANE患者有严重神经后遗症。包括类固醇治疗和IVIG在内的早期治疗与较好预后无关。需要进一步研究以建立ANE管理的共识指南。