Jędrusik Piotr, Symonides Bartosz, Lewandowski Jacek, Gaciong Zbigniew
Department of Internal Medicine, Hypertension and Vascular Diseases, Medical University of Warsaw, Warsaw, Poland.
Front Pharmacol. 2021 May 13;12:684111. doi: 10.3389/fphar.2021.684111. eCollection 2021.
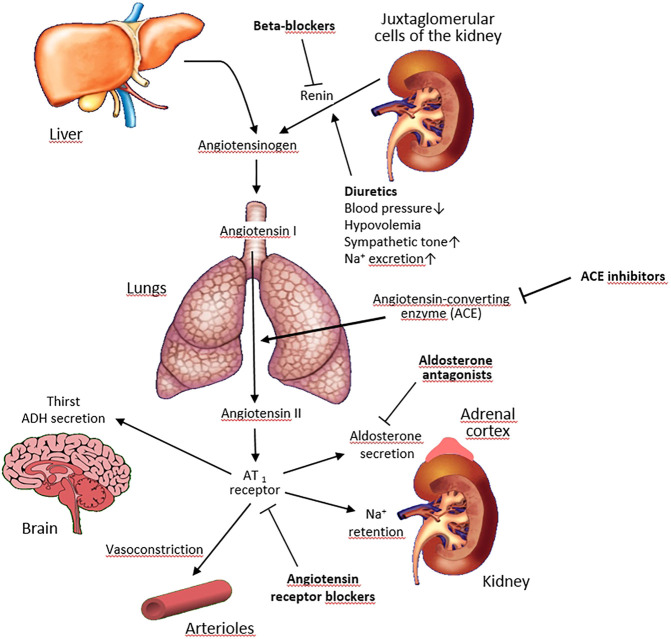
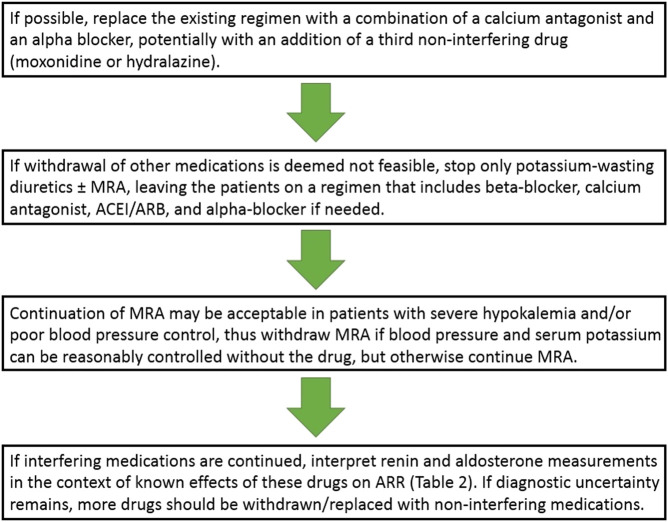
Primary aldosteronism (PA) is a potentially curable form of secondary hypertension caused by excessive renin-independent aldosterone secretion, leading to increased target organ damage and cardiovascular morbidity and mortality. The diagnosis of PA requires measuring renin and aldosterone to calculate the aldosterone-to-renin ratio, followed by confirmatory tests to demonstrate renin-independent aldosterone secretion and/or PA subtype differentiation. Various antihypertensive drug classes interfere with the renin-angiotensin-aldosterone axis and hence evaluation for PA should ideally be performed off-drugs. This is, however, often precluded by the risks related to suboptimal control of blood pressure and serum potassium level in the evaluation period. In the present review, we summarized the evidence regarding the effect of various antihypertensive drug classes on biochemical testing for PA, and critically appraised the issue whether and which antihypertensive medications should be withdrawn or, conversely, might be continued in patients evaluated for PA. The least interfering drugs are calcium antagonists, alpha-blockers, hydralazine, and possibly moxonidine. If necessary, the testing may also be attempted during treatment with beta-blockers, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers but renin and aldosterone measurements must be interpreted in the context of known effects of these drugs on these parameters. Views are evolving on the feasibility of testing during treatment with mineralocorticoid receptor antagonists, as these drugs are now increasingly considered acceptable in specific patient subsets, particularly in those with severe hypokalemia and/or poor blood pressure control on alternative treatment.
原发性醛固酮增多症(PA)是一种由肾素非依赖性醛固酮分泌过多引起的继发性高血压,可潜在治愈,会导致靶器官损害增加以及心血管疾病的发病率和死亡率上升。PA的诊断需要测量肾素和醛固酮以计算醛固酮与肾素比值,随后进行确诊试验以证实肾素非依赖性醛固酮分泌和/或PA亚型鉴别。各类抗高血压药物会干扰肾素 - 血管紧张素 - 醛固酮轴,因此PA的评估理想情况下应在停药状态下进行。然而,在评估期间,由于血压和血清钾水平控制不佳带来的风险,这一点往往难以做到。在本综述中,我们总结了各类抗高血压药物对PA生化检测影响的相关证据,并审慎评估了在PA评估患者中是否以及应停用哪些抗高血压药物,或者相反,哪些药物可能可以继续使用的问题。干扰最小的药物是钙拮抗剂、α受体阻滞剂、肼屈嗪,可能还有莫索尼定。如有必要,在使用β受体阻滞剂、血管紧张素转换酶抑制剂和血管紧张素受体阻滞剂治疗期间也可尝试进行检测,但肾素和醛固酮测量结果必须结合这些药物对这些参数的已知影响来解读。对于在使用盐皮质激素受体拮抗剂治疗期间进行检测的可行性,观点正在不断演变,因为现在越来越多的特定患者亚组,特别是那些患有严重低钾血症和/或在替代治疗中血压控制不佳的患者,认为这些药物是可以接受的。