Zhu Yinggang, Monsel Antoine, Roberts Jason A, Pontikis Konstantinos, Mimoz Olivier, Rello Jordi, Qu Jieming, Rouby Jean-Jacques
Department of Pulmonary and Critical Care Medicine, Hua-Dong Hospital, Fudan University, Shanghai 200433, China.
Multidisciplinary Intensive Care Unit, Department of Anaesthesiology and Critical Care, La Pitié-Salpêtrière Hospital, Assistance Publique Hôpitaux de Paris, Medicine Sorbonne University, 75012 Paris, France.
Microorganisms. 2021 May 27;9(6):1154. doi: 10.3390/microorganisms9061154.
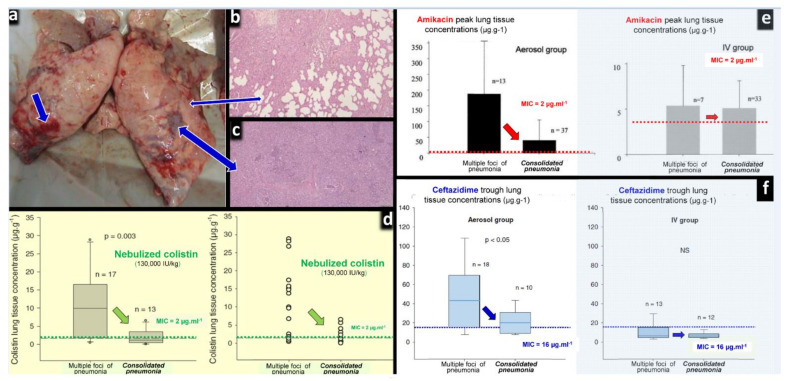
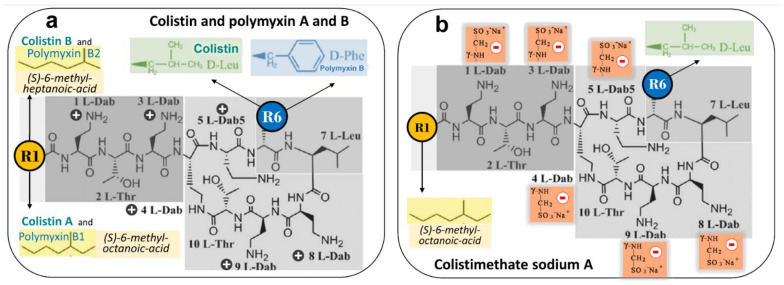
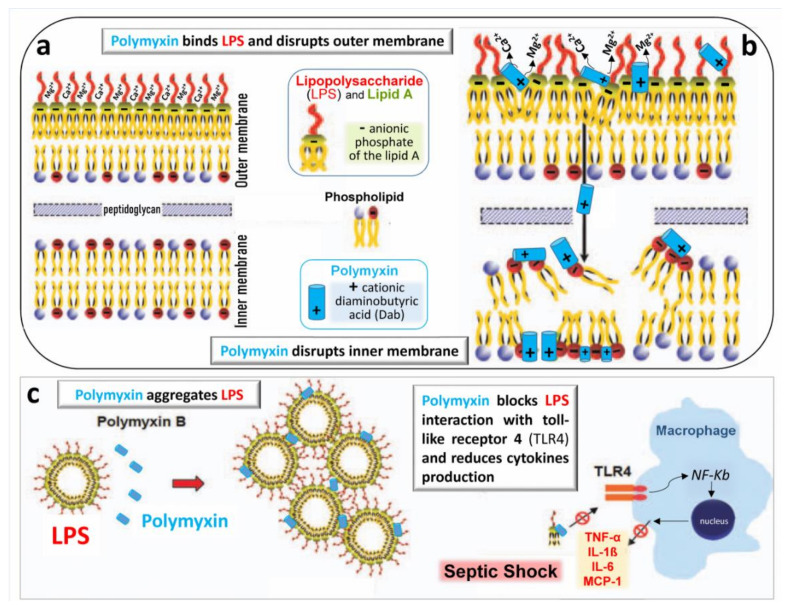
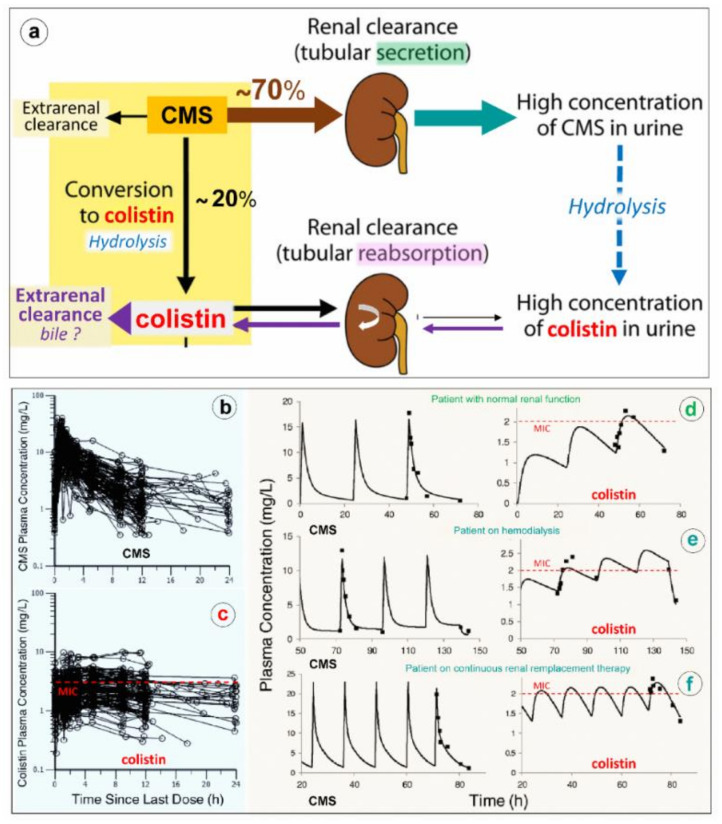
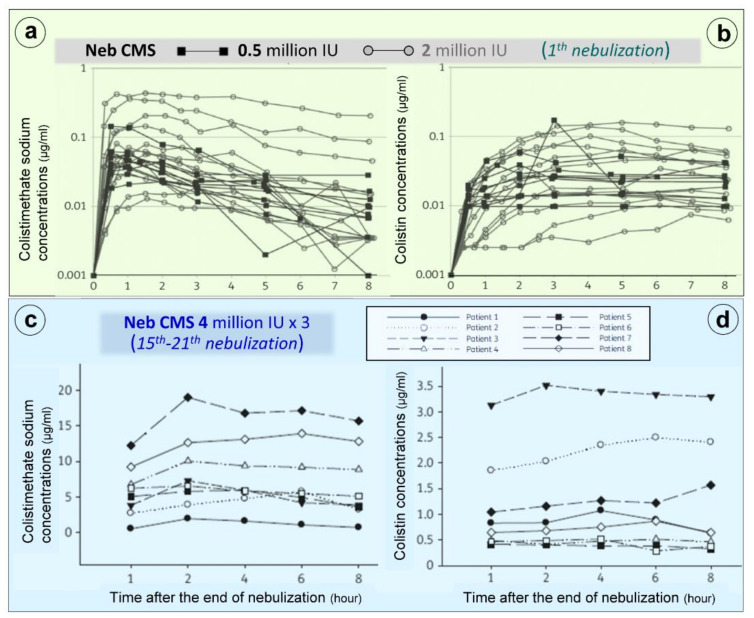
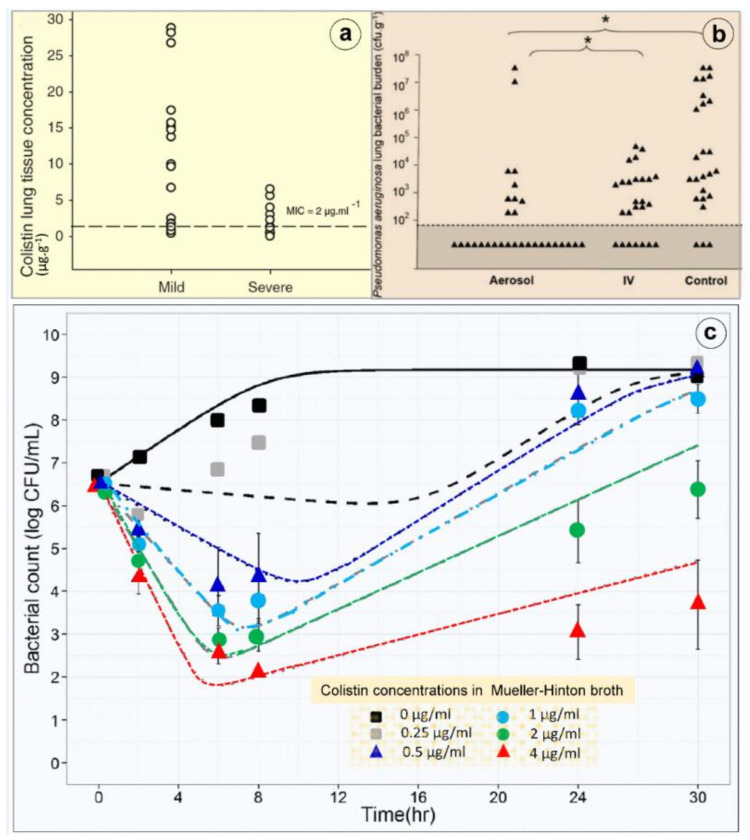
Clinical evidence suggests that nebulized colistimethate sodium (CMS) has benefits for treating lower respiratory tract infections caused by multidrug-resistant Gram-negative bacteria (GNB). Colistin is positively charged, while CMS is negatively charged, and both have a high molecular mass and are hydrophilic. These physico-chemical characteristics impair crossing of the alveolo-capillary membrane but enable the disruption of the bacterial wall of GNB and the aggregation of the circulating lipopolysaccharide. Intravenous CMS is rapidly cleared by glomerular filtration and tubular excretion, and 20-25% is spontaneously hydrolyzed to colistin. Urine colistin is substantially reabsorbed by tubular cells and eliminated by biliary excretion. Colistin is a concentration-dependent antibiotic with post-antibiotic and inoculum effects. As CMS conversion to colistin is slower than its renal clearance, intravenous administration can lead to low plasma and lung colistin concentrations that risk treatment failure. Following nebulization of high doses, colistin (200,000 international units/24h) lung tissue concentrations are > five times minimum inhibitory concentration (MIC) of GNB in regions with multiple foci of bronchopneumonia and in the range of MIC breakpoints in regions with confluent pneumonia. Future research should include: (1) experimental studies using lung microdialysis to assess the PK/PD in the interstitial fluid of the lung following nebulization of high doses of colistin; (2) superiority multicenter randomized controlled trials comparing nebulized and intravenous CMS in patients with pandrug-resistant GNB ventilator-associated pneumonia and ventilator-associated tracheobronchitis; (3) non-inferiority multicenter randomized controlled trials comparing nebulized CMS to intravenous new cephalosporines/ß-lactamase inhibitors in patients with extensive drug-resistant GNB ventilator-associated pneumonia and ventilator-associated tracheobronchitis.
临床证据表明,雾化吸入多粘菌素甲磺酸钠(CMS)对治疗由多重耐药革兰氏阴性菌(GNB)引起的下呼吸道感染有益。多粘菌素带正电荷,而CMS带负电荷,两者分子量都很高且具有亲水性。这些物理化学特性会妨碍其穿过肺泡毛细血管膜,但能破坏GNB的细胞壁并使循环中的脂多糖聚集。静脉注射CMS会通过肾小球滤过和肾小管排泄迅速清除,20% - 25%会自发水解为多粘菌素。尿液中的多粘菌素会被肾小管细胞大量重吸收,并通过胆汁排泄消除。多粘菌素是一种浓度依赖性抗生素,具有抗生素后效应和接种物效应。由于CMS转化为多粘菌素的速度比其肾脏清除速度慢,静脉给药会导致血浆和肺组织中的多粘菌素浓度较低,有治疗失败的风险。高剂量雾化吸入后,在支气管肺炎多病灶区域,肺组织中的多粘菌素(200,000国际单位/24小时)浓度大于GNB最低抑菌浓度(MIC)的5倍,在融合性肺炎区域则处于MIC折点范围内。未来的研究应包括:(1)使用肺微透析的实验研究,以评估高剂量多粘菌素雾化吸入后肺间质液中的药代动力学/药效学;(2)在泛耐药GNB呼吸机相关性肺炎和呼吸机相关性气管支气管炎患者中比较雾化吸入和静脉注射CMS的优效性多中心随机对照试验;(3)在广泛耐药GNB呼吸机相关性肺炎和呼吸机相关性气管支气管炎患者中比较雾化吸入CMS与静脉注射新型头孢菌素/β-内酰胺酶抑制剂的非劣效性多中心随机对照试验。