Department of Radiation Oncology, University of California, Los Angeles, Los Angeles, CA, USA.
Cancer Med. 2021 Jul;10(14):4734-4742. doi: 10.1002/cam4.4028. Epub 2021 Jun 2.
Though utilization of medical procedures has been shown to vary considerably across the United States, similar efforts to characterize variation in the delivery of radiation therapy (RT) procedures have not been forthcoming. Our aim was to characterize variation in the delivery of common RT procedures in the Medicare population. We hypothesized that delivery would vary significantly based on provider characteristics.
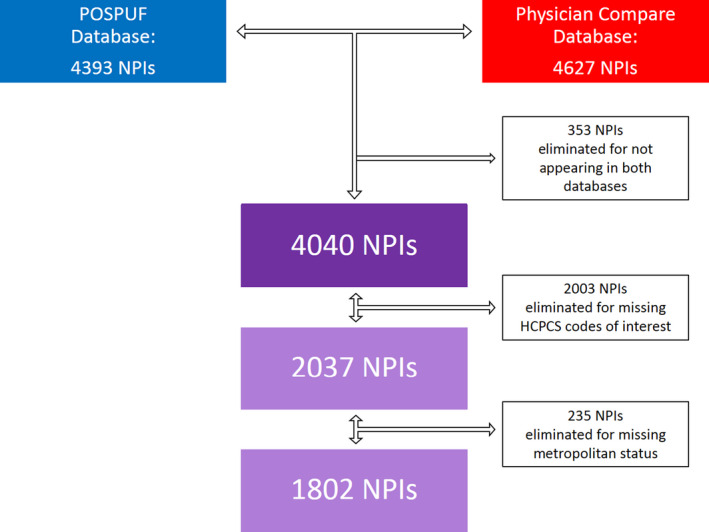
The Centers for Medicare and Medicaid Services (CMS) Physician and Other Supplier Public Use File was linked to the CMS Physician Compare (PC) database by physician NPI to identify and sum all treatment delivery charges submitted by individual radiation oncologists in the non-facility-based (NFB) setting in 2016. Multivariable logistic regression analysis was carried out to determine provider characteristics (gender, practice rurality, practice region, and years since graduation) that predicted for the delivery of 3D conformal RT (3DCRT), intensity modulated RT (IMRT), stereotactic body RT (SBRT), stereotactic radiosurgery (SRS), low dose rate (LDR) brachytherapy, and high dose rate (HDR) brachytherapy delivery in the Medicare patient population. The overall significance of categorical variables in the multivariable logistic regression model was assessed by the likelihood ratio test (LRT).
In total, 1,802 physicians from the NFB practice setting were analyzed. Male gender predicted for greater LDR brachytherapy delivery (OR 8.19, 95% CI 2.58-26.05, p < 0.001), but not greater delivery of other technologies. Metropolitan practice was the only predictor for greater HDR brachytherapy utilization (OR 12.95, 95% CI 1.81-92.60, p = 0.01). Practice region was predictive of the delivery of 3DCRT, SRS and SBRT (p < 0.01, p < 0.001, and p < 0.001, respectively). With the Northeast as the reference region, 3DCRT was more likely to be delivered by providers in the South (OR 1.33, 95% CI 1.09-1.62, p < 0.01) and the West (OR 1.38, 95% CI 1.11-1.71, p < 0.01). At the same time, SRS use was less likely in the Midwest (OR 0.71, 95% CI 0.55-0.91, p < 0.01), South (OR 0.49, 95% CI 0.40-0.61, p < 0.001), and West (OR 0.43, 95% CI 0.34-0.55, p < 0.001). SBRT, on the other hand, was more commonly utilized in the Midwest (OR 2.63, 95% CI 1.13-6.13, p = 0.03), South (OR 3.44, 95% CI 1.58-7.49, p < 0.01), and West (OR 4.87, 95% CI 2.21-10.72, p < 0.001). HDR brachytherapy use was also more likely in the Midwest (OR 1.97, 95% CI 1.11-3.49, p = 0.02) and West (OR 1.87, 95% CI 1.08-3.24, p = 0.03). While the degree held by the billing physician did not predict for delivery of a given procedure, greater years since graduation was related to decreased likelihood of SBRT use (OR 0.98, 95% CI 0.96-0.99, p < 0.001) and increased likelihood of LDR brachytherapy use (OR 1.02, 95% CI 1.00-1.04, p = 0.02).
Substantial geographic variation in the use of specific RT technologies was identified. The degree to which this variation reflects effective care, preference-sensitive care, or supply-sensitive care warrants further investigation.
尽管已经证实美国各地的医疗程序利用情况存在很大差异,但尚未有类似的努力来描述放射治疗(RT)程序的提供情况。我们的目的是描述医疗保险人群中常见 RT 程序的提供情况。我们假设提供情况会根据提供者的特征而有很大差异。
将医疗保险和医疗补助服务中心(CMS)医生和其他供应商公共使用文件与 CMS 医生比较(PC)数据库通过医生 NPI 链接,以识别和汇总 2016 年非设施基础(NFB)环境中每位放射肿瘤学家提交的所有治疗交付费用。进行多变量逻辑回归分析,以确定预测 Medicare 患者人群中 3D 适形 RT(3DCRT)、强度调制 RT(IMRT)、立体定向体 RT(SBRT)、立体定向放射外科(SRS)、低剂量率(LDR)近距离放射治疗和高剂量率(HDR)近距离放射治疗的提供者特征(性别、实践农村性、实践地区和毕业后年限)。通过似然比检验(LRT)评估多变量逻辑回归模型中分类变量的整体显著性。
总共分析了来自 NFB 实践环境的 1802 名医生。男性性别预测 LDR 近距离放射治疗的使用更高(OR 8.19,95%CI 2.58-26.05,p<0.001),但其他技术的使用则没有增加。大都市实践是唯一预测 HDR 近距离放射治疗利用率更高的因素(OR 12.95,95%CI 1.81-92.60,p=0.01)。实践地区预测了 3DCRT、SRS 和 SBRT 的使用(p<0.01,p<0.001 和 p<0.001,分别)。以东北部为参考区域,3DCRT 更可能由南部(OR 1.33,95%CI 1.09-1.62,p<0.01)和西部(OR 1.38,95%CI 1.11-1.71,p<0.01)的提供者提供。与此同时,在中西部(OR 0.71,95%CI 0.55-0.91,p<0.01)、南部(OR 0.49,95%CI 0.40-0.61,p<0.001)和西部(OR 0.43,95%CI 0.34-0.55,p<0.001),SRS 的使用则更少。另一方面,SBRT 在中西部(OR 2.63,95%CI 1.13-6.13,p=0.03)、南部(OR 3.44,95%CI 1.58-7.49,p<0.01)和西部(OR 4.87,95%CI 2.21-10.72,p<0.001)中更常见。HDR 近距离放射治疗的使用在中西部(OR 1.97,95%CI 1.11-3.49,p=0.02)和西部(OR 1.87,95%CI 1.08-3.24,p=0.03)也更高。虽然计费医生的学位水平没有预测特定程序的使用,但毕业后年限的增加与 SBRT 使用的可能性降低(OR 0.98,95%CI 0.96-0.99,p<0.001)和 LDR 近距离放射治疗使用的可能性增加(OR 1.02,95%CI 1.00-1.04,p=0.02)有关。
确定了特定 RT 技术使用的大量地理差异。这种差异在多大程度上反映了有效护理、偏好敏感护理还是供应敏感护理,需要进一步研究。