Department of Orthopedics, Affiliated Hospital of Southwest Medical University, No. 25 Taiping Street, Sichuan, 646000, Luzhou, China.
Sichuan Provincial Laboratory of Orthopedic Engineering, No. 25 Taiping Street, Sichuan, 646000, Luzhou, China.
BMC Musculoskelet Disord. 2021 Jun 2;22(1):510. doi: 10.1186/s12891-021-04394-3.
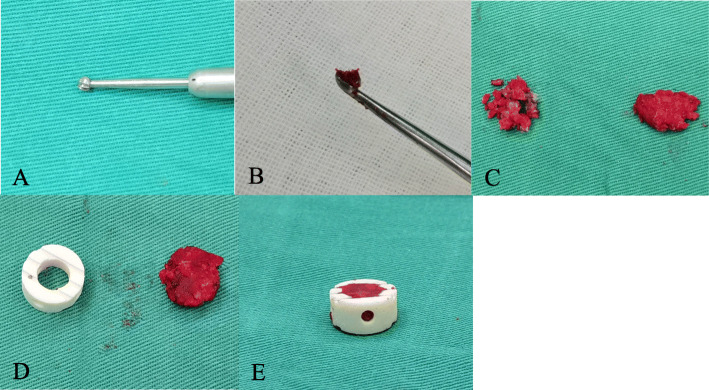
Using a cage filled with local bone in anterior cervical discectomy and fusion (ACDF) can eliminate morbidities associated with autograft harvest from the iliac crest while achieving high fusion rates. However, there is still no consensus regarding the methods for using local bone grafts. This retrospective study was performed to compare the clinical and radiological outcomes of using a mixture of bone dust and morselized bone versus morselized bone alone in ACDF.
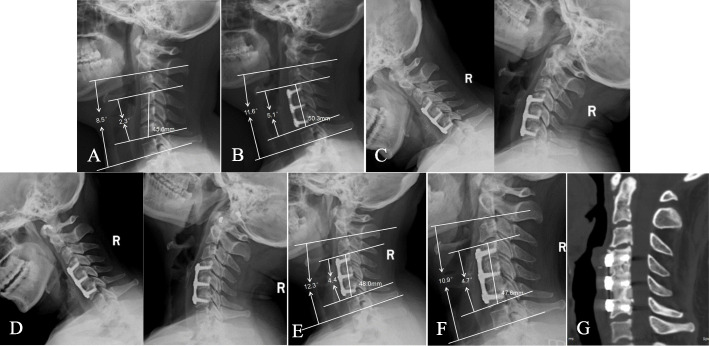
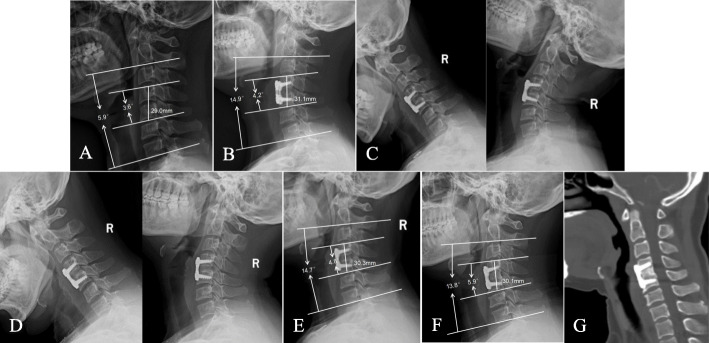
A retrospective study of 228 patients affected by cervical degenerative disease who had undergone single- or double-level ACDF between January 2014 and June 2018 was performed. Nanohydroxyapatite/polyamide-66 (n-HA/PA66) combined with morselized bone was used in 111 patients (group A: single-level ACDF in 51 patients and double-level ACDF in 60 patients), whereas the n-HA/PA66 cage combined with a mixture of bone dust and morselized bone was used in 117 patients (group B: single-level ACDF in 58 patients and double-level ACDF in 59 patients). The fusion rate, extent of cage subsidence, fusion segmental height (FSH), C2-7 lordosis, segmental sagittal alignment (SSA), 10-point visual analog scale (VAS) score, and Neck Disability Index (NDI) were compared between the two groups.
The VAS score and NDI were significantly reduced after the operation in group A and group B. At the final follow-up, the fusion rate was 90.2 % (46/51) and 94.8 % (55/58) in patients treated with single-level ACDF in group A and group B, respectively (p > 0.05). In patients treated with double-level ACDF, bone fusion was achieved in 52 patients (86.7 %) in group A and 55 patients (93.2 %) in group B (p > 0.05). The fusion rate of single- and double-level ACDF was higher in patients in group B than those in group A at the 3-month, 6-month and 12-month follow-ups (p < 0.05). The extent of cage subsidence after single- and double-level ACDF was lower in patients in group B (1.5 ± 0.5 mm and 2.3 ± 0.8 mm, respectively) than in those in group A (1.8 ± 0.7 mm and 2.9 ± 1.4 mm, respectively) (p < 0.05). There was no significant difference between the two groups in the C2-7 lordosis, FSH, SSA, VAS score, or NDI before or after the operation (p > 0.05).
Using a mixture of local bone dust and morselized bone as cage-filling materials yielded comparably good clinical outcomes as using morselized bone alone in single- and double-level ACDF. However, the mixture graft of bone dust and morselized bone was more beneficial in promoting early fusion and reducing cage subsidence.
在颈椎前路椎间盘切除融合术(ACDF)中使用充满自体骨的椎间融合器可以消除取自髂嵴的自体移植物相关的发病率,同时实现高融合率。然而,对于使用自体骨移植物的方法仍没有共识。本回顾性研究旨在比较在 ACDF 中使用骨屑和碎骨与仅使用碎骨混合物的临床和影像学结果。
回顾性研究了 2014 年 1 月至 2018 年 6 月期间接受单节段或双节段 ACDF 的 228 例患有颈椎退行性疾病的患者。纳米羟基磷灰石/聚酰胺-66(n-HA/PA66)与碎骨联合使用于 111 例患者(A 组:51 例单节段 ACDF,60 例双节段 ACDF),而 n-HA/PA66 椎间融合器与骨屑和碎骨的混合物联合使用于 117 例患者(B 组:58 例单节段 ACDF,59 例双节段 ACDF)。比较两组之间的融合率、椎间融合器下沉程度、融合节段高度(FSH)、C2-7 后凸、节段矢状位排列(SSA)、10 分视觉模拟评分(VAS)和颈椎功能障碍指数(NDI)。
A 组和 B 组患者在手术后 VAS 评分和 NDI 均明显降低。在最终随访时,A 组和 B 组单节段 ACDF 治疗的患者的融合率分别为 90.2%(46/51)和 94.8%(55/58)(p>0.05)。在双节段 ACDF 治疗的患者中,A 组有 52 例(86.7%)和 B 组有 55 例(93.2%)患者达到骨融合(p>0.05)。在单节段和双节段 ACDF 治疗的患者中,B 组患者在术后 3 个月、6 个月和 12 个月的随访中融合率均高于 A 组(p<0.05)。B 组患者单节段和双节段 ACDF 术后的椎间融合器下沉程度(1.5±0.5mm 和 2.3±0.8mm)均低于 A 组(1.8±0.7mm 和 2.9±1.4mm)(p<0.05)。两组患者在手术前后的 C2-7 后凸、FSH、SSA、VAS 评分和 NDI 均无统计学差异(p>0.05)。
在单节段和双节段 ACDF 中,使用骨屑和碎骨混合物作为椎间融合器填充材料与单独使用碎骨具有相当的临床效果。然而,骨屑和碎骨混合移植物更有利于促进早期融合和减少椎间融合器下沉。