Ye Zhikang, Wang Ying, Ge Long, Guyatt Gordon H, Collister David, Alhazzani Waleed, Bagshaw Sean M, Belley-Cote Emilie P, Fang Fang, Hou Liangying, Kolb Philipp, Lamontagne Francois, Oczkowski Simon, Pyne Lonnie, Rabbat Christian, Scaum Matt, Najafabadi Borna Tadayon, Tangamornsuksan Wimonchat, Wald Ron, Wang Qi, Walsh Michael, Yao Liang, Zeng Linan, Algarni Abdullah Mohammed, Couban Rachel J, Alexander Paul Elias, Rochwerg Bram
Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, ON, Canada.
Evidence Based Social Science Research Center, School of Public Health, Lanzhou University, Lanzhou, China.
Crit Care Explor. 2021 May 12;3(5):e0399. doi: 10.1097/CCE.0000000000000399. eCollection 2021 May.
To compare different modalities of renal replacement therapy in critically ill adults with acute kidney injury.
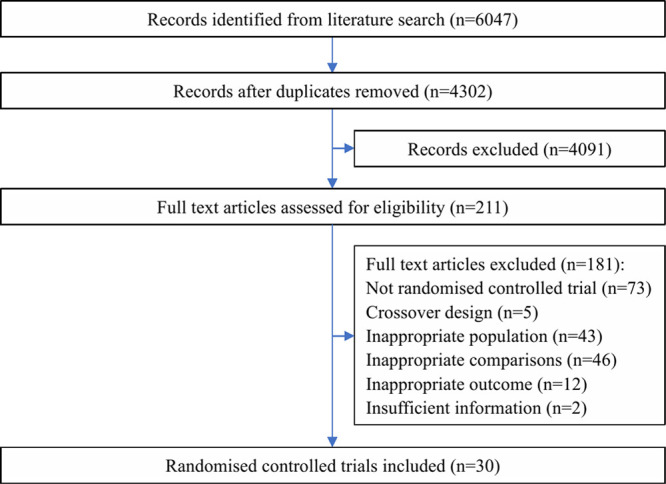
We searched Medline, PubMed, Embase, Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov from inception to 25 May, 2020. We included randomized controlled trials comparing the efficacy and safety of different renal replacement therapy modalities in critically ill patients with acute kidney injury.
Ten reviewers (working in pairs) independently screened studies for eligibility, extracted data, and assessed risk of bias.
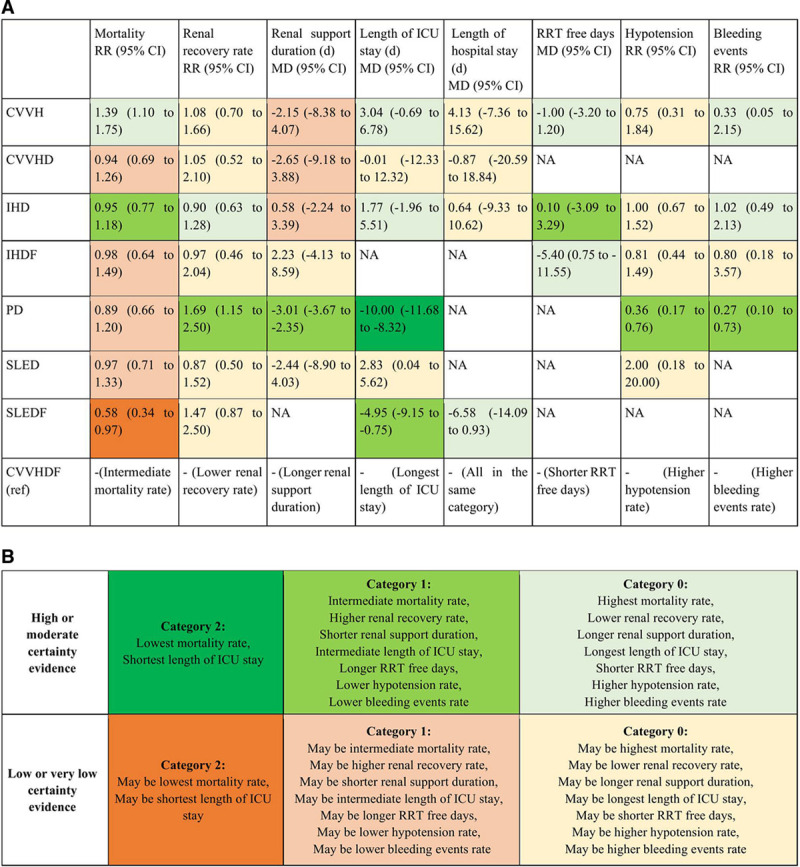
We performed random-effects frequentist network meta-analyses and used the Grading of Recommendations, Assessment, Development, and Evaluation approach to assess certainty of evidence. The primary analysis was a four-node analysis: continuous renal replacement therapy, intermittent hemodialysis, slow efficiency extended dialysis, and peritoneal dialysis. The secondary analysis subdivided these four nodes into nine nodes including continuous veno-venous hemofiltration, continuous veno-venous hemodialysis, continuous veno-venous hemodiafiltration, continuous arterio-venous hemodiafiltration, intermittent hemodialysis, intermittent hemodialysis with hemofiltration, slow efficiency extended dialysis, slow efficiency extended dialysis with hemofiltration, and peritoneal dialysis. We set the minimal important difference threshold for mortality as 2.5% (relative difference, 0.04).
Thirty randomized controlled trials ( = 3,774 patients) proved eligible. There may be no difference in mortality between continuous renal replacement therapy and intermittent hemodialysis (relative risk, 1.04; 95% CI, 0.93-1.18; low certainty), whereas continuous renal replacement therapy demonstrated a possible increase in mortality compared with slow efficiency extended dialysis (relative risk, 1.06; 95% CI, 0.85-1.33; low certainty) and peritoneal dialysis (relative risk, 1.16; 95% CI, 0.92-1.49; low certainty). Continuous renal replacement therapy may increase renal recovery compared with intermittent hemodialysis (relative risk, 1.15; 95% CI, 0.91-1.45; low certainty), whereas both continuous renal replacement therapy and intermittent hemodialysis may be worse for renal recovery compared with slow efficiency extended dialysis and peritoneal dialysis (low certainty). Peritoneal dialysis was probably associated with the shortest duration of renal support and length of ICU stay compared with other interventions (low certainty for most comparisons). Slow efficiency extended dialysis may be associated with shortest length of hospital stay (low or moderate certainty for all comparisons) and days of mechanical ventilation (low certainty for all comparisons) compared with other interventions. There was no difference between continuous renal replacement therapy and intermittent hemodialysis in terms of hypotension (relative risk, 0.92; 95% CI, 0.72-1.16; moderate certainty) or other complications of therapy, but an increased risk of hypotension and bleeding was seen with both modalities compared with peritoneal dialysis (low or moderate certainty). Complications of slow efficiency extended dialysis were not sufficiently reported to inform comparisons.
The results of this network meta-analysis suggest there is no difference in mortality between continuous renal replacement therapy and intermittent hemodialysis although continuous renal replacement therapy may increases renal recovery compared with intermittent hemodialysis. Slow efficiency extended dialysis with hemofiltration may be the most effective intervention at reducing mortality. Peritoneal dialysis is associated with good efficacy, and the least number of complications however may not be practical in all settings. Importantly, all conclusions are based on very low to moderate certainty evidence, limited by imprecision. At the very least, ICU clinicians should feel comfortable that the differences between continuous renal replacement therapy, intermittent hemodialysis, slow efficiency extended dialysis, and, where clinically appropriate, peritoneal dialysis are likely small, and any of these modalities is a reasonable option to employ in critically ill patients.
比较危重症急性肾损伤成人患者不同的肾脏替代治疗方式。
我们检索了从创建至2020年5月25日的Medline、PubMed、Embase、Cochrane对照试验中央注册库和ClinicalTrials.gov。我们纳入了比较不同肾脏替代治疗方式在危重症急性肾损伤患者中的疗效和安全性的随机对照试验。
十名评审员(两人一组)独立筛选研究以确定其是否符合条件、提取数据并评估偏倚风险。
我们进行了随机效应频率学派网状Meta分析,并使用推荐分级、评估、制定和评价方法来评估证据的确定性。主要分析是四节点分析:连续性肾脏替代治疗、间歇性血液透析、缓慢低效延长透析和腹膜透析。次要分析将这四个节点细分为九个节点,包括连续性静脉-静脉血液滤过、连续性静脉-静脉血液透析、连续性静脉-静脉血液透析滤过、连续性动脉-静脉血液透析滤过、间歇性血液透析、血液滤过的间歇性血液透析、缓慢低效延长透析、血液滤过的缓慢低效延长透析和腹膜透析。我们将死亡率的最小重要差异阈值设定为2.5%(相对差异,0.04)。
30项随机对照试验(n = 3774例患者)被证明符合条件。连续性肾脏替代治疗和间歇性血液透析之间的死亡率可能没有差异(相对风险,1.04;95%可信区间,0.93 - 1.18;低确定性),而与缓慢低效延长透析相比,连续性肾脏替代治疗显示死亡率可能增加(相对风险,1.06;95%可信区间,0.85 - 1.33;低确定性),与腹膜透析相比也是如此(相对风险,1.16;95%可信区间,0.92 - 1.49;低确定性)。与间歇性血液透析相比,连续性肾脏替代治疗可能提高肾脏恢复率(相对风险,1.15;95%可信区间,0.91 - 1.45;低确定性),而与缓慢低效延长透析和腹膜透析相比,连续性肾脏替代治疗和间歇性血液透析在肾脏恢复方面可能都较差(低确定性)。与其他干预措施相比,腹膜透析可能与最短的肾脏支持时间和ICU住院时间相关(大多数比较为低确定性)。与其他干预措施相比,缓慢低效延长透析可能与最短的住院时间(所有比较为低或中等确定性)和机械通气天数(所有比较为低确定性)相关。连续性肾脏替代治疗和间歇性血液透析在低血压(相对风险,0.92;95%可信区间,0.72 - 1.16;中等确定性)或其他治疗并发症方面没有差异,但与腹膜透析相比,这两种方式都有低血压和出血风险增加(低或中等确定性)。缓慢低效延长透析的并发症报告不足,无法进行比较。
这项网状Meta分析的结果表明,连续性肾脏替代治疗和间歇性血液透析之间的死亡率没有差异,尽管与间歇性血液透析相比,连续性肾脏替代治疗可能提高肾脏恢复率。血液滤过的缓慢低效延长透析可能是降低死亡率最有效的干预措施。腹膜透析疗效良好,并发症最少,但可能并非在所有情况下都可行。重要的是,所有结论都基于非常低到中等确定性的证据,受不精确性限制。至少,ICU临床医生应该放心,连续性肾脏替代治疗、间歇性血液透析、缓慢低效延长透析以及在临床合适时的腹膜透析之间的差异可能很小,这些方式中的任何一种在危重症患者中都是合理的选择。