Hussain Shabbir, Hafeez Abdul, Nazim Hira, Gohar Rahim, Mallick Muhammad Jawaid
Oncology, Ziauddin University, Karachi, PAK.
Oncology, Aga Khan University Hospital, Nairobi, KEN.
Cureus. 2021 Apr 28;13(4):e14744. doi: 10.7759/cureus.14744.
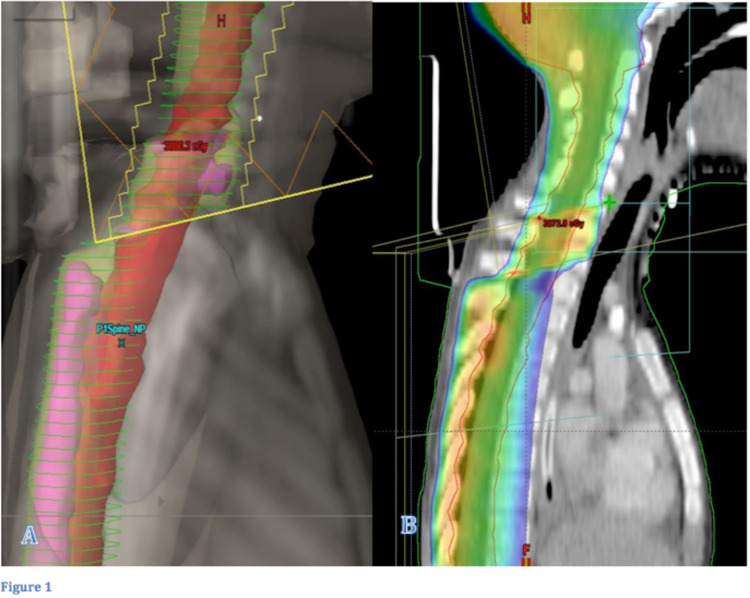
Planning craniospinal irradiation (CSI) with ''field-in-field'' (FIF) homogenization technique in combination with daily, intrafractional modulation of the field junctions is needed to avoid spinal cord overdose. Photon-based techniques for CSI may result in dose inhomogeneity within the treatment volume and usually require a weekly manual shift of the field junctions to minimize the possibility of spinal cord overdose. Nowadays, FIF technique is used to feather out the dose inhomogeneity caused by multiple fields. We have started using this technique after acquiring advanced technology machines in recent years.
Sixteen patients treated with three-dimensional conformal radiation therapy (3D-CRT) for CSI were retrospectively chosen for analysis. These patients were treated during 2019-2020. Contouring of planning target volume (PTV) and organs at risk (OAR) was done, and planning was done on Varian Eclipse Treatment Planning System (TPS) (Varian Medical Systems, Palo Alto, CA). These patients were planned with lateral craniocervical fields and posterior spinal fields using a forward-planned FIF technique. Field junctions were automatically modulated and custom-weighted for maximal homogeneity within each treatment fraction. Dose-volume histogram (DVH) was used for analysis of results. A corresponding plan without FIF technique was planned; then maximum dose at the junction was noted for each patient with both plans, and the readings were evaluated. Paired sample t-test was used to compute the p-values for the inferential statistics.
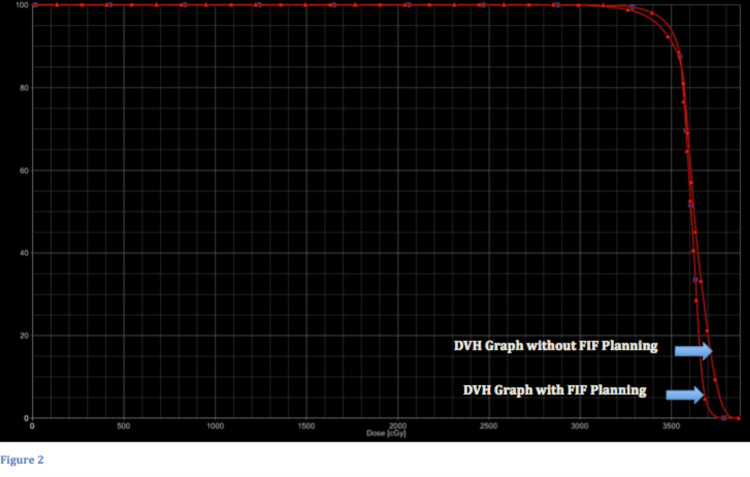
Without FIF technique, the volume receiving 110% of the prescribed dose ranged from 39% to 74% (mean: 62.12%) and volume receiving 120% dose ranged from 8% to 28% (mean: 17.68%), whereas with FIF technique, the thecal sac volume receiving 110% of dose ranged from 2% to 18% (mean: 11%) and volume receiving 120% ranged from 0% to 2%. Volume receiving 100% of the dose was also calculated in both techniques; mean values of this dose range was almost similar in both groups. Later p-value was calculated, and in both dose ranges of thecal sac volume receiving 110% and 120%, the difference in values was statistically significant. Therefore, it proved that plan inhomogeneity improved with FIF technique. This technique provided consistent dose delivery during each fraction of treatment across the junctions. The maximum doses calculated at the junction were higher in the CSI plans without FIF compared to those with FIF technique.
This study concludes that better dose homogeneity is achieved with FIF technique as compared to non-FIF technique, and the difference in values was statistically significant.
采用“野中野”(FIF)匀化技术并结合每日野衔接的分次内调制来计划全脑全脊髓照射(CSI),以避免脊髓剂量过高。基于光子的CSI技术可能会导致治疗体积内的剂量不均匀,并且通常需要每周手动移动野衔接以尽量减少脊髓剂量过高的可能性。如今,FIF技术用于消除多野引起的剂量不均匀。近年来在购置了先进技术设备后,我们开始使用该技术。
回顾性选取16例接受三维适形放疗(3D-CRT)治疗CSI的患者进行分析。这些患者于2019年至2020年期间接受治疗。对计划靶区(PTV)和危及器官(OAR)进行轮廓勾画,并在瓦里安Eclipse治疗计划系统(TPS)(瓦里安医疗系统公司,加利福尼亚州帕洛阿尔托)上进行计划。这些患者采用前向计划的FIF技术,使用侧位颅颈野和后脊髓野进行计划。对野衔接进行自动调制并定制权重,以在每个治疗分次内实现最大程度的均匀性。使用剂量体积直方图(DVH)分析结果。计划了一个不使用FIF技术的相应计划;然后记录两个计划中每位患者在野衔接处的最大剂量,并对读数进行评估。使用配对样本t检验计算推断统计的p值。
在不使用FIF技术时,接受处方剂量110%的体积范围为39%至74%(平均:62.12%),接受120%剂量的体积范围为8%至28%(平均:17.68%),而使用FIF技术时,接受剂量110%的脊髓腔体积范围为2%至18%(平均:11%),接受120%剂量的体积范围为0%至2%。两种技术还计算了接受100%剂量的体积;该剂量范围的平均值在两组中几乎相似。随后计算p值,在脊髓腔体积接受110%和120%剂量的两个范围内,数值差异均具有统计学意义。因此,证明使用FIF技术可改善计划的不均匀性。该技术在治疗的每个分次中跨野衔接提供了一致的剂量输送。与使用FIF技术的CSI计划相比,不使用FIF技术的CSI计划在野衔接处计算出的最大剂量更高。
本研究得出结论,与非FIF技术相比,FIF技术可实现更好的剂量均匀性,且数值差异具有统计学意义。