Choudhary Rishabh C, Shoaib Muhammad, Sohnen Samantha, Rolston Daniel M, Jafari Daniel, Miyara Santiago J, Hayashida Kei, Molmenti Ernesto P, Kim Junhwan, Becker Lance B
Laboratory for Critical Care Physiology, The Feinstein Institutes for Medical Research, Northwell Health, Manhasset, NY, United States.
Department of Emergency Medicine, Northshore University Hospital, Northwell Health, Manhasset, NY, United States.
Front Med (Lausanne). 2021 May 18;8:636651. doi: 10.3389/fmed.2021.636651. eCollection 2021.
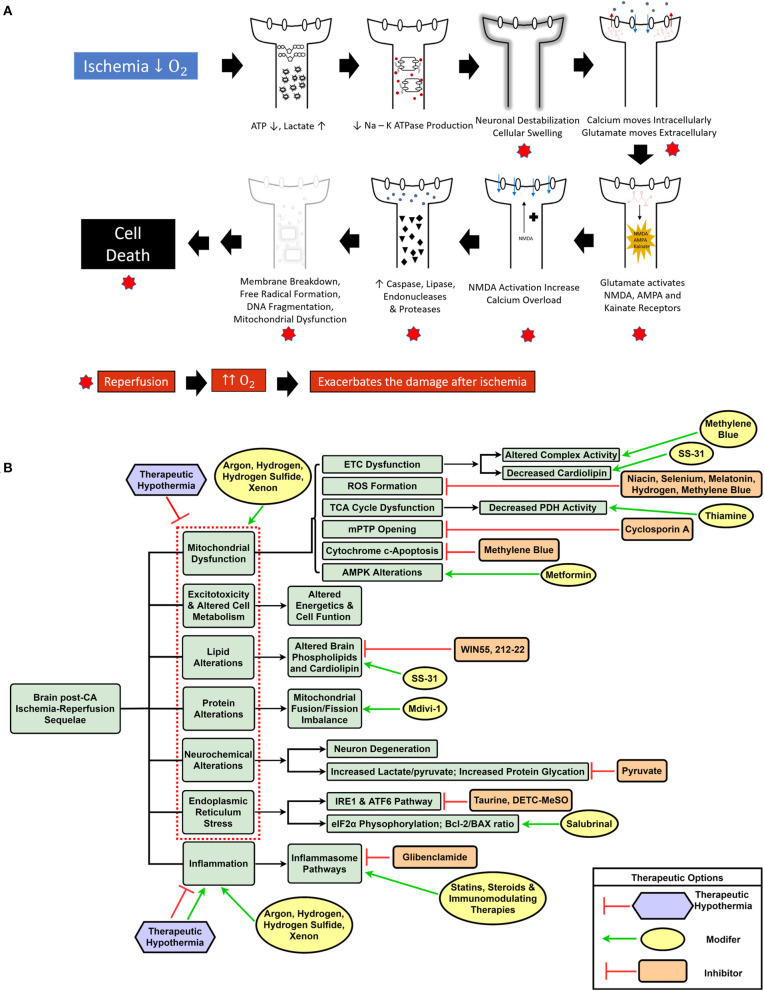
Cardiac arrest (CA) results in global ischemia-reperfusion injury damaging tissues in the whole body. The landscape of therapeutic interventions in resuscitation medicine has evolved from focusing solely on achieving return of circulation to now exploring options to mitigate brain injury and preserve brain function after CA. CA pathology includes mitochondrial damage and endoplasmic reticulum stress response, increased generation of reactive oxygen species, neuroinflammation, and neuronal excitotoxic death. Current non-pharmacologic therapies, such as therapeutic hypothermia and extracorporeal cardiopulmonary resuscitation, have shown benefits in protecting against ischemic brain injury and improving neurological outcomes post-CA, yet their application is difficult to institute ubiquitously. The current preclinical pharmacopeia to address CA and the resulting brain injury utilizes drugs that often target singular pathways and have been difficult to translate from the bench to the clinic. Furthermore, the limited combination therapies that have been attempted have shown mixed effects in conferring neuroprotection and improving survival post-CA. The global scale of CA damage and its resultant brain injury necessitates the future of CA interventions to simultaneously target multiple pathways and alleviate the hemodynamic, mitochondrial, metabolic, oxidative, and inflammatory processes in the brain. This narrative review seeks to highlight the current field of post-CA neuroprotective pharmaceutical therapies, both singular and combination, and discuss the use of an extensive multi-drug cocktail therapy as a novel approach to treat CA-mediated dysregulation of multiple pathways, enhancing survival, and neuroprotection.
心脏骤停(CA)会导致全身性缺血再灌注损伤,损害全身组织。复苏医学中的治疗干预格局已从单纯关注恢复循环发展到现在探索减轻CA后脑损伤和保护脑功能的方法。CA病理包括线粒体损伤和内质网应激反应、活性氧生成增加、神经炎症和神经元兴奋性毒性死亡。目前的非药物疗法,如治疗性低温和体外心肺复苏,已显示出在预防缺血性脑损伤和改善CA后神经学结果方面的益处,但其应用难以普遍实施。目前用于解决CA及其导致的脑损伤的临床前药典使用的药物通常针对单一途径,并且难以从实验室转化到临床。此外,已尝试的有限联合疗法在提供神经保护和改善CA后生存率方面显示出混合效果。CA损伤及其导致的脑损伤的全球规模使得CA干预的未来需要同时针对多个途径,并减轻大脑中的血流动力学、线粒体、代谢、氧化和炎症过程。这篇叙述性综述旨在突出当前CA后神经保护药物治疗领域,包括单一药物和联合药物,并讨论使用广泛的多药鸡尾酒疗法作为一种新颖的方法来治疗CA介导的多种途径失调、提高生存率和神经保护。