Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York, USA.
Division of Cardiology, Department of Internal Medicine, Weill Cornell Medical College, New York Presbyterian Hospital, New York, New York, USA.
Heart Lung. 2021 Sep-Oct;50(5):618-621. doi: 10.1016/j.hrtlng.2021.04.010. Epub 2021 May 27.
To evaluate the association between pre-hospitalization antiplatelet medication use and COVID-19 disease severity.
Retrospective cohort study.
Inpatient units at The Mount Sinai Hospital.
Adults age ≥18 admitted between March 1, 2020 and April 9, 2020 with confirmed COVID-19 infection with at least 28 days follow-up.
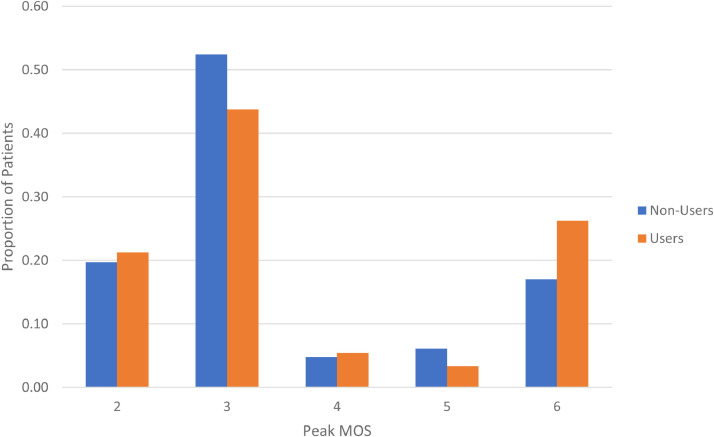
We captured baseline demographic, pre-hospitalization antiplatelet medication use, and clinical encounter data for all patients who met inclusion criteria. The primary endpoint was peak score on a 6-point modified ordinal scale (MOS), which is based on World Health Organization blueprint R&S groups, used to grade severity of illness through clinical outcomes of interest. Scores indicate the following: 1 - COVID-19 infection not requiring hospitalization, 2 - requiring hospitalization but not supplemental oxygen, 3 - hospitalization requiring supplemental oxygen, 4 - hospitalization requiring high-flow nasal cannula (HFNC) or non-invasive positive pressure ventilation (NIPPV), 5 - hospitalization requiring intubation or extracorporeal membrane oxygenation (ECMO), 6 - death. Multivariable adjusted partial proportional odds model (PPOM) was performed to examine the association between pre-hospitalization antiplatelet medication use and likelihood of each MOS score.
Of 762 people admitted with COVID-19, 239 (31.4%) used antiplatelet medications pre-hospitalization while 523 (68.6%) did not. Antiplatelet users were older and had more co-morbidities at baseline. Before adjusting for covariates, patients who used antiplatelet medications pre-hospitalization were more likely than non-users to have peak MOS score 6 (death, OR 1.75, 95% CI 1.21-2.52), peak MOS score ≥5 (intubation/ECMO or death, OR 1.4, 95% CI 1.00-1.98) and peak MOS score ≥4 (HFNC, NIPPV, intubation/ECMO or death, OR 1.40, 95% CI 1.01-1.94). On multivariable adjusted PPOM analysis controlling for 13 covariates, there were no longer any significant differences in peak MOS scores between users and non-users.
After adjusting for covariates, pre-hospital antiplatelet use was not associated with COVID-19 severity in hospitalized patients.
评估住院前抗血小板药物使用与 COVID-19 疾病严重程度的关系。
回顾性队列研究。
西奈山医院的住院病房。
2020 年 3 月 1 日至 2020 年 4 月 9 日期间,年龄≥18 岁的因确诊 COVID-19 感染而住院的成年人,且至少有 28 天的随访。
我们为所有符合纳入标准的患者采集了基线人口统计学、住院前抗血小板药物使用情况和临床就诊数据。主要终点是基于世界卫生组织蓝图 R&S 组的 6 分改良等级量表(MOS)的峰值评分,该量表用于根据感兴趣的临床结果对疾病严重程度进行分级。评分表明:1-不需要住院的 COVID-19 感染,2-需要住院但不需要补充氧气,3-需要补充氧气的住院,4-需要高流量鼻导管(HFNC)或无创正压通气(NIPPV)的住院,5-需要插管或体外膜氧合(ECMO)的住院,6-死亡。采用多变量调整部分比例优势模型(PPOM)来检验住院前抗血小板药物使用与 MOS 评分每个等级的可能性之间的关联。
在 762 名因 COVID-19 住院的患者中,有 239 人(31.4%)在住院前使用了抗血小板药物,而 523 人(68.6%)没有。抗血小板药物使用者年龄更大,且在基线时合并症更多。在调整协变量之前,与非使用者相比,使用住院前抗血小板药物的患者更有可能出现 MOS 评分 6 (死亡,OR 1.75,95%CI 1.21-2.52)、MOS 评分≥5(插管/ECMO 或死亡,OR 1.4,95%CI 1.00-1.98)和 MOS 评分≥4(HFNC、NIPPV、插管/ECMO 或死亡,OR 1.40,95%CI 1.01-1.94)。在多变量调整后的 PPOM 分析中,控制了 13 个协变量后,使用者和非使用者之间的 MOS 评分峰值没有差异。
在调整协变量后,住院前使用抗血小板药物与住院 COVID-19 患者的严重程度无关。