University of California San Diego, La Jolla, CA.
University of Utah, Salt Lake City, UT and Intermountain Healthcare, Inc., Murray, UT.
Chest. 2021 Nov;160(5):1822-1831. doi: 10.1016/j.chest.2021.05.052. Epub 2021 Jun 4.
The United States Chronic Thromboembolic Pulmonary Hypertension Registry (US-CTEPH-R) was designed to characterize the demographic characteristics, evaluation, clinical course, and outcomes of surgical and nonsurgical therapies for patients with chronic thromboembolic pulmonary hypertension.
What are the differences in baseline characteristics and 1-year outcomes between operated and nonoperated subjects?
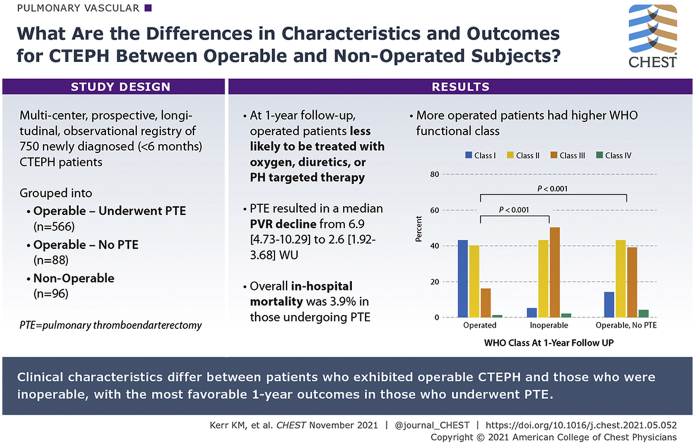
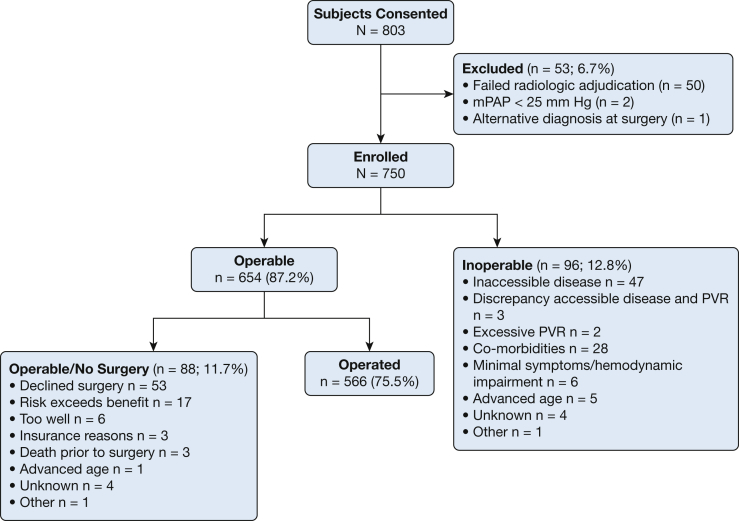
This study describes a multicenter, prospective, longitudinal, observational registry of patients newly diagnosed (< 6 months) with CTEPH. Inclusion criteria required a mean pulmonary artery pressure ≥ 25 mm Hg documented by right heart catheterization and radiologic confirmation of CTEPH. Between 2015 and 2018, a total of 750 patients were enrolled and followed up biannually until 2019.
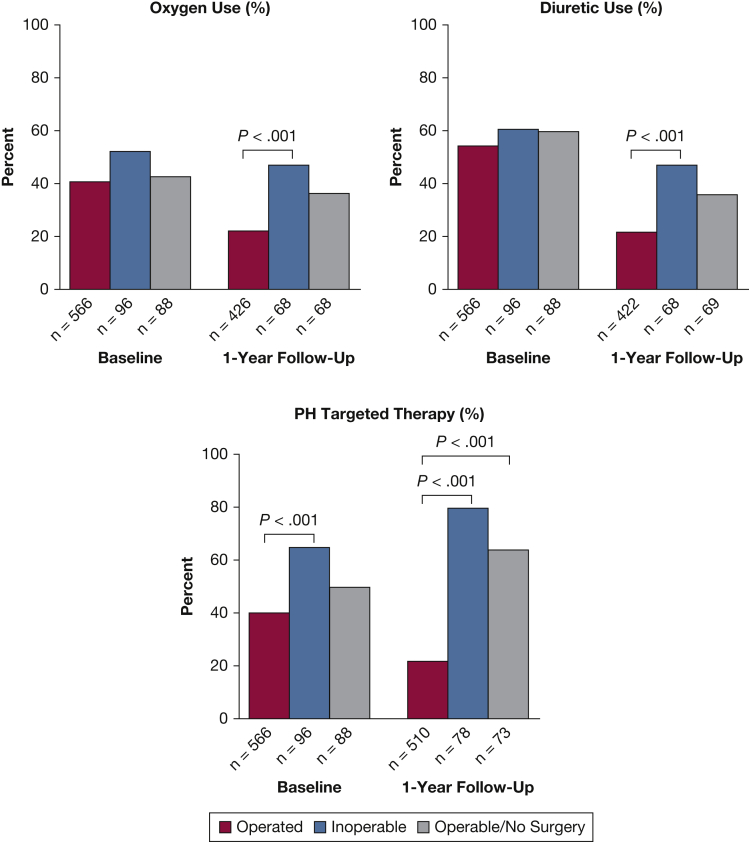
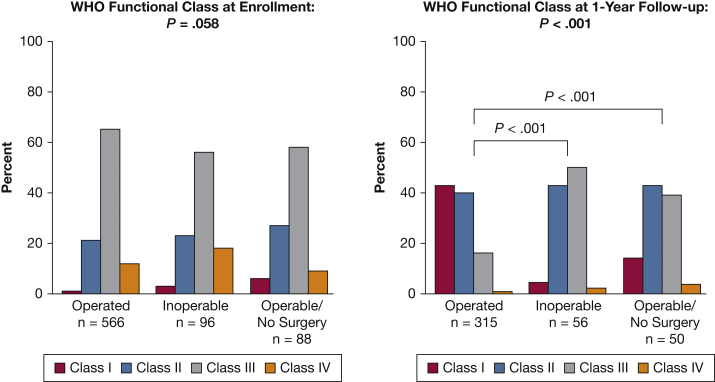
Most patients with CTEPH (87.9%) reported a history of acute pulmonary embolism. CTEPH diagnosis delays were frequent (median, 10 months), and most patients reported World Health Organization functional class 3 status at enrollment with a median mean pulmonary artery pressure of 44 mm Hg. The registry cohort was subdivided into Operable patients undergoing pulmonary thromboendarterectomy (PTE) surgery (n = 566), Operable patients who did not undergo surgery (n = 88), and those who were Inoperable (n = 96). Inoperable patients were older than Operated patients; less likely to be obese; have a DVT history, non-type O blood group, or thrombophilia; and more likely to have COPD or a history of cancer. PTE resulted in a median pulmonary vascular resistance decline from 6.9 to 2.6 Wood units (P < .001) with a 3.9% in-hospital mortality. At 1-year follow-up, Operated patients were less likely treated with oxygen, diuretics, or pulmonary hypertension-targeted therapy compared with Inoperable patients. A larger percentage of Operated patients were World Health Organization functional class 1 or 2 at 1 year (82.9%) compared with the Inoperable (48.2%) and Operable/No Surgery (56%) groups (P < .001).
Differences exist in the clinical characteristics between patients who exhibited operable CTEPH and those who were inoperable, with the most favorable 1-year outcomes in those who underwent PTE surgery.
ClinicalTrials.gov; No.: NCT02429284; URL: www.clinicaltrials.gov.
美国慢性血栓栓塞性肺动脉高压注册研究(US-CTEPH-R)旨在描述手术和非手术治疗慢性血栓栓塞性肺动脉高压患者的人口统计学特征、评估、临床过程和结局。
手术和未手术患者的基线特征和 1 年结局有何差异?
本研究描述了一项新诊断(<6 个月)的 CTEPH 患者多中心、前瞻性、纵向、观察性注册研究。纳入标准要求平均肺动脉压≥25mmHg,并通过右心导管检查和 CTEPH 的放射学确认。在 2015 年至 2018 年间,共纳入了 750 例患者,并每两年随访一次,直到 2019 年。
大多数 CTEPH 患者(87.9%)有急性肺栓塞病史。CTEPH 诊断延迟很常见(中位数为 10 个月),大多数患者在入组时报告为世界卫生组织功能分类 3 级,平均肺动脉压为 44mmHg。该注册研究队列分为接受肺动脉血栓内膜切除术(PTE)手术的可手术患者(n=566)、未接受手术的可手术患者(n=88)和不可手术患者(n=96)。不可手术患者比手术患者年龄更大;不太可能肥胖;有深静脉血栓形成史、非 O 型血或血栓形成倾向;更有可能患有 COPD 或癌症。PTE 可使肺血管阻力中位数从 6.9 降至 2.6 伍德单位(P<0.001),住院死亡率为 3.9%。在 1 年随访时,与不可手术患者相比,手术患者更不可能接受氧疗、利尿剂或肺动脉高压靶向治疗。1 年时,更多的手术患者处于世界卫生组织功能分类 1 级或 2 级(82.9%),而不可手术患者(48.2%)和可手术/未手术患者(56%)比例较低(P<0.001)。
可手术 CTEPH 患者和不可手术患者之间存在临床特征差异,接受 PTE 手术的患者 1 年结局最佳。
ClinicalTrials.gov;编号:NCT02429284;网址:www.clinicaltrials.gov。