Chuaychoosakoon Chaiwat, Suwannaphisit Sitthiphong
Department of Orthopedics, Faculty of Medicine, Prince of Songkla University, Hat Yai, Thailand.
Orthop J Sports Med. 2021 May 20;9(5):23259671211008834. doi: 10.1177/23259671211008834. eCollection 2021 May.
The axillary nerve is at risk for iatrogenic injuries in surgical procedures involving the lateral aspect of the shoulder joint. To date and to our knowledge, there have been no studies that have compared the relevant distances in the common arm abduction positions used in these types of surgery as well as the relative risks of each position.
To evaluate the effect of arm abduction position on the distance from the acromion process to the axillary nerve in the common abducted arm positions.
Descriptive laboratory study.
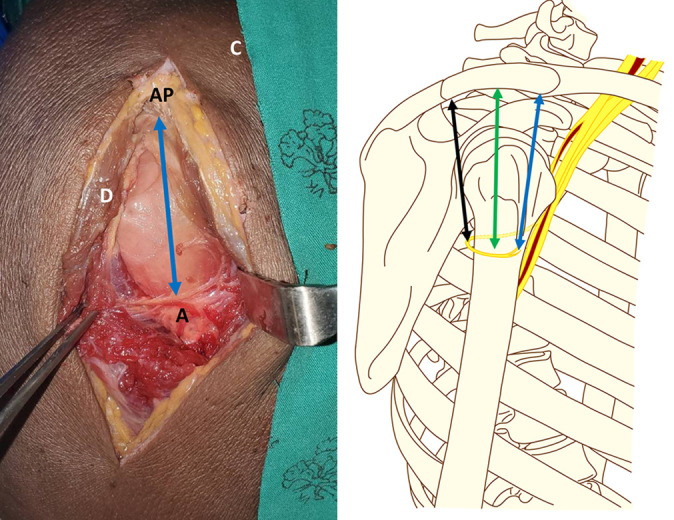
The shoulders of 10 fresh-frozen, full-body cadaveric specimens were used. A saber incision was made at the anterolateral edge of the acromion, and the anterior branch of the axillary nerve was identified. The distance between the anterolateral edge of the acromion process and the axillary nerve was measured 3 times in each of 4 positions: with the arm at the side as well as at 30°, 60°, and 90° of abduction. Then, the same procedure was performed from the midlateral and the posterolateral edges of the acromion process. The distances of the acromion process to the axillary nerve in the 4 positions were compared using 2-way analysis of variance.
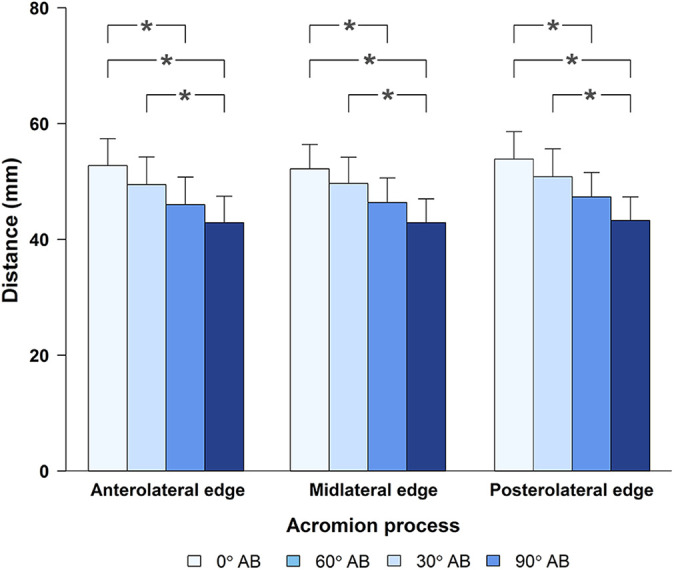
The mean distances from the anterolateral edge of the acromion process to the anterior branch of the axillary nerve were 52.76 ± 4.64 mm with the arm at the side, 49.48 ± 4.77 mm at 30° of abduction, 46.00 ± 4.75 mm at 60° of abduction, and 42.88 ± 4.59 mm at 90° of abduction. There was a significant decrease in the distance from the anterolateral edge of the acromion process to the axillary nerve as the abduction angle of the arm increased from 0° to 60°, 0° to 90°, and 30° to 90° ( < .05).
The distances from the acromion process to the axillary nerve were shorter in all abducted arm positions than with the arm at the side.
To avoid iatrogenic axillary nerve injuries, surgeons should be aware of the safe zone based on the shortest distance from the acromion process to the axillary nerve to ensure no accidental damage to this structure instead of using the mean distance of 5 cm.
在涉及肩关节外侧的外科手术中,腋神经有发生医源性损伤的风险。据我们所知,迄今为止尚无研究比较这类手术中常用的手臂外展位置的相关距离以及每个位置的相对风险。
评估手臂外展位置对常见外展手臂位置时肩峰至腋神经距离的影响。
描述性实验室研究。
使用10具新鲜冷冻的全身尸体标本的肩部。在肩峰前外侧边缘做一个剑形切口,识别腋神经前支。在4个位置分别测量肩峰前外侧边缘与腋神经之间的距离3次:手臂位于身体一侧以及外展30°、60°和90°时。然后,从肩峰的中外侧和后外侧边缘进行相同的操作。使用双向方差分析比较4个位置时肩峰至腋神经的距离。
手臂位于身体一侧时,肩峰前外侧边缘至腋神经前支的平均距离为52.76±4.64mm,外展30°时为49.48±4.77mm,外展60°时为46.00±4.75mm,外展90°时为42.88±4.59mm。随着手臂外展角度从0°增加到60°、0°增加到90°以及30°增加到90°,肩峰前外侧边缘至腋神经的距离显著减小(P<0.05)。
所有手臂外展位置时肩峰至腋神经的距离均比手臂位于身体一侧时短。
为避免医源性腋神经损伤,外科医生应根据肩峰至腋神经的最短距离知晓安全区域,以确保不会意外损伤该结构,而不是使用5cm的平均距离。