Department of Radiation Oncology, University of California Los Angeles, 200 Medical Plaza Driveway, Suite B265, Los Angeles, CA, 90095, USA.
Department of Radiology Thoracic Interventional Services, University of California Los Angeles, Los Angeles, CA, 90095, USA.
Radiat Oncol. 2021 Jun 7;16(1):99. doi: 10.1186/s13014-021-01826-1.
Centrally located lung tumors present treatment challenges given their proximity to mediastinal structures including the central airway, esophagus, major vessels, and heart. Therapeutic options can be limited for medically inoperable patients, particularly if they have received previous thoracic radiotherapy. High dose rate (HDR) brachyablation was developed to improve the therapeutic ratio for patients with central lung tumors. The purpose of this study is to report initial safety and efficacy outcomes with this treatment for central lung malignancies.
From September 2015 to August 2019, a total of 25 patients with 37 pulmonary tumors were treated with percutaneous HDR brachyablation. Treatment was delivered by a multi-disciplinary team of interventional radiologists, pulmonologists, and radiation oncologists. Twenty-three patients received a median dose of 21.5 Gy (range 15-27.5) in a single fraction, whereas two patients received median dose of 24.75 Gy (range 24-25.5) over 2-3 fractions. Tumor local control (LC) was evaluated by Response Evaluation Criteria in Solid Tumors v1.1. Treatment-related toxicities were graded by Common Terminology Criteria for Adverse Events v5.0, with adverse events less than 90 days defined as acute, and those occurring later were defined as late. LC, progression-free survival (PFS), and overall survival (OS) rates were estimated by the Kaplan-Meier method.
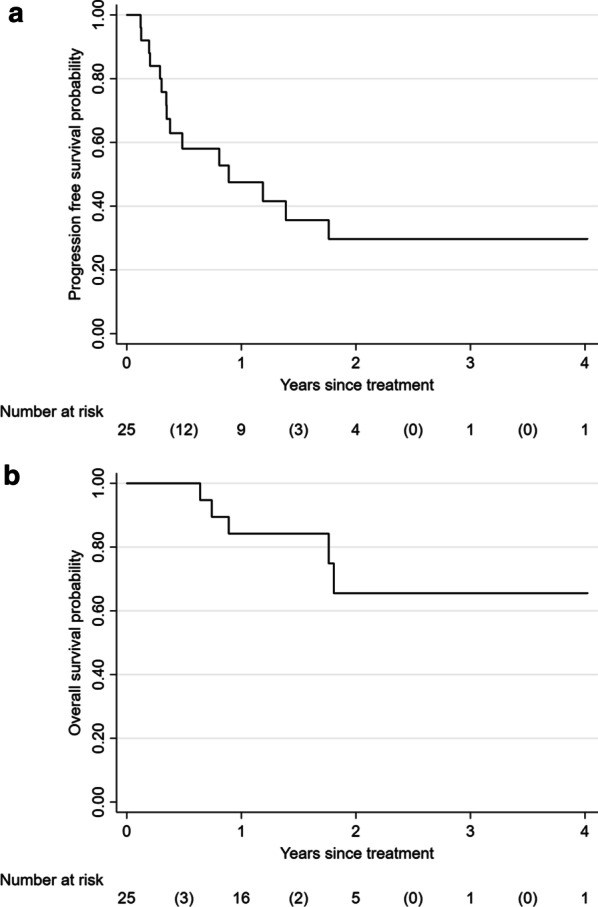
Of 37 treated tumors, 88% were metastatic. Tumor location was central and ultra-central in 24.3% and 54.1%, respectively. Average tumor volume was 11.6 cm (SD 12.4, range 0.57-62.8). Median follow-up was 19 months (range 3-48). Two-year LC, PFS, and OS were 96.2%, 29.7%, and 65.5%, respectively. Thirteen of 39 (33.3%) catheter implantation procedures were associated with trace minor pneumothorax requiring no intervention, 1 (2.5%) procedure with minor radiographic pulmonary hemorrhage, and 4 (10.3%) with major pneumothorax requiring chest tube insertions. All procedural complications resolved within 24 h from treatment. Acute grade 1-2 toxicity was identified in 4 patients, whereas none developed late toxicity beyond 90 days of follow-up.
Percutaneous HDR brachyablation is a safe and promising treatment option for centrally located primary and metastatic lung tumors. Future comparisons with stereotactic body radiotherapy and other ablative techniques are warranted to expand multi-disciplinary management options.
由于中央气道、食管、大血管和心脏等纵隔结构的临近,中央型肺肿瘤的治疗极具挑战性。对于不能进行手术的患者,治疗方案可能会受到限制,特别是如果他们之前接受过胸部放疗。高剂量率(HDR)近距离放疗的发展旨在提高中央型肺肿瘤患者的治疗效果。本研究旨在报告这种治疗中央型肺癌的初步安全性和疗效结果。
从 2015 年 9 月到 2019 年 8 月,共有 25 名患者的 37 个肺部肿瘤接受了经皮 HDR 近距离放疗。治疗由介入放射科医生、肺病学家和放射肿瘤学家组成的多学科团队实施。23 名患者接受了单次中位剂量 21.5 Gy(范围 15-27.5)的治疗,而 2 名患者接受了中位剂量 24.75 Gy(范围 24-25.5)的 2-3 次分割治疗。通过实体瘤反应评估标准 1.1 评估肿瘤局部控制(LC)。采用通用不良事件术语标准 5.0 对治疗相关毒性进行分级,90 天内发生的不良事件定义为急性,90 天后发生的不良事件定义为晚期。通过 Kaplan-Meier 法估计 LC、无进展生存期(PFS)和总生存期(OS)。
37 个治疗肿瘤中,88%为转移性肿瘤。肿瘤位置分别为中央和超中央,分别占 24.3%和 54.1%。平均肿瘤体积为 11.6 cm(SD 12.4,范围 0.57-62.8)。中位随访时间为 19 个月(范围 3-48)。2 年 LC、PFS 和 OS 分别为 96.2%、29.7%和 65.5%。39 例导管植入术中有 13 例(33.3%)与需要干预的微量气胸相关,1 例(2.5%)与轻微放射性肺出血相关,4 例(10.3%)与需要插入胸腔引流管的严重气胸相关。所有程序并发症均在治疗后 24 小时内得到解决。4 名患者出现 1-2 级急性毒性,而无 1 名患者在 90 天随访后出现晚期毒性。
经皮 HDR 近距离放疗是治疗中央型原发性和转移性肺癌的一种安全且有前途的治疗选择。未来有必要与立体定向体部放疗和其他消融技术进行比较,以扩大多学科治疗方案。