Discovery Medicine, GlaxoSmithKline R&D, GSK House, Brentford, UK.
Global Clinical Operations, GlaxoSmithKline, GSK House, Brentford, UK.
Int J Chron Obstruct Pulmon Dis. 2021 Jun 3;16:1637-1646. doi: 10.2147/COPD.S309320. eCollection 2021.
Management of acute exacerbations of chronic obstructive pulmonary disease (COPD) is sometimes inadequate leading to either prolonged duration and/or an increased risk of recurrent exacerbations in the period following the initial event.
To evaluate the safety and efficacy of inhaled nemiralisib, a phosphoinositide 3-kinase δ inhibitor, in patients experiencing an acute exacerbation of COPD.
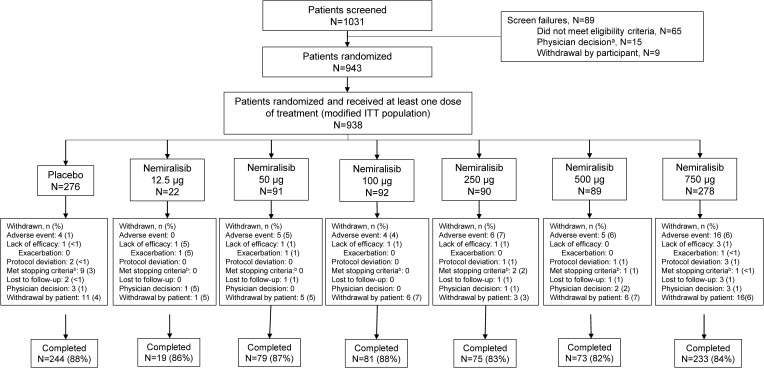
In this double-blind, placebo-controlled study, COPD patients (40-80 years, ≥10 pack-year smoking history, current moderate/severe acute exacerbation of COPD requiring standard-of-care treatment) were randomized to placebo or nemiralisib 12.5 µg, 50 µg, 100 µg, 250 µg, 500 µg, or 750 µg (ratio of 3:1:1:1:1:1:3; N=938) for 12 weeks with an exploratory 12-week follow-up period. The primary endpoint was change from baseline in post-bronchodilator FEV at week 12. Key secondary endpoints were rate of re-exacerbations, patient-reported outcomes (Exacerbations of Chronic Pulmonary Disease Tool, COPD Assessment Test, St George's Respiratory Questionnaire-COPD), plasma pharmacokinetics (PK) and safety/tolerability.
There was no difference in change from baseline FEV at week 12 between the nemiralisib and placebo treatment groups (posterior adjusted median difference, nemiralisib 750 µg and placebo: -0.004L (95% CrI: -0.051L to 0.042L)). Overall, there were also no differences between nemiralisib and placebo in secondary endpoints, including re-exacerbations. Plasma PK increased in a dose proportional manner. The most common adverse event for nemiralisib was post-inhalation cough which appeared to be dose-related.
The addition of nemiralisib to standard-of-care treatment for 12 weeks did not improve lung function or re-exacerbations in patients with, and following an acute exacerbation of COPD. However, this study demonstrated that large clinical trials recruiting acutely exacerbating patients can successfully be conducted.
慢性阻塞性肺疾病(COPD)急性加重的管理有时并不充分,导致初始事件后,病程延长和/或再次加重的风险增加。
评估吸入性磷酸肌醇 3-激酶 δ 抑制剂 nemiralisib 治疗 COPD 急性加重患者的安全性和疗效。
在这项双盲、安慰剂对照研究中,将 40-80 岁、有≥10 包年吸烟史、目前处于需要标准治疗的中重度 COPD 急性加重期的 COPD 患者随机分为安慰剂或 nemiralisib 12.5μg、50μg、100μg、250μg、500μg、750μg(3:1:1:1:1:1:3 比例;N=938),治疗 12 周,并进行 12 周的探索性随访期。主要终点为 12 周时支气管扩张剂后 FEV1 的基线变化。关键次要终点为再加重率、患者报告的结局(慢性阻塞性肺病工具、COPD 评估测试、圣乔治呼吸问卷-COPD)、血浆药代动力学(PK)和安全性/耐受性。
在 nemiralisib 和安慰剂治疗组之间,第 12 周时 FEV1 的基线变化无差异(后调整的中位数差值,nemiralisib 750μg 和安慰剂:-0.004L(95%可信区间:-0.051L 至 0.042L))。总体而言,在次要终点方面,包括再加重,nemiralisib 和安慰剂之间也没有差异。PK 呈剂量依赖性增加。nemiralisib 最常见的不良事件是吸入后咳嗽,似乎与剂量有关。
在标准治疗的基础上加用 nemiralisib 治疗 12 周,并未改善 COPD 急性加重和之后患者的肺功能或再加重。然而,这项研究表明,可成功开展招募急性加重患者的大型临床试验。