Saxena Kapil, Jabbour Elias, Issa Ghayas, Sasaki Koji, Ravandi Farhad, Maiti Abhishek, Daver Naval, Kadia Tapan, DiNardo Courtney D, Konopleva Marina, Cortes Jorge E, Yilmaz Musa, Chien Kelly, Pierce Sherry, Kantarjian Hagop, Short Nicholas J
Division of Cancer Medicine, MD Anderson Cancer Center, Houston, TX, USA.
Department of Leukemia, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Unit 0428, Houston, TX, 77030, USA.
J Hematol Oncol. 2021 Jun 15;14(1):94. doi: 10.1186/s13045-021-01106-1.
The natural course of untreated chronic myeloid leukemia (CML) is progression to an aggressive blast phase. Even in the current era of BCR-ABL1 tyrosine kinase inhibitors (TKIs), the outcomes of blast phase CML remain poor with no consensus frontline treatment approach.
We retrospectively analyzed the response rates and survival outcomes of 104 consecutive patients with myeloid blast phase CML (CML-MBP) treated from 2000 to 2019 based on 4 different frontline treatment approaches: intensive chemotherapy (IC) + TKI (n = 20), hypomethylating agent (HMA) + TKI (n = 20), TKI alone (n = 56), or IC alone (n = 8). We also evaluated the impact of TKI selection and subsequent allogeneic stem cell transplant (ASCT) on patient outcomes.
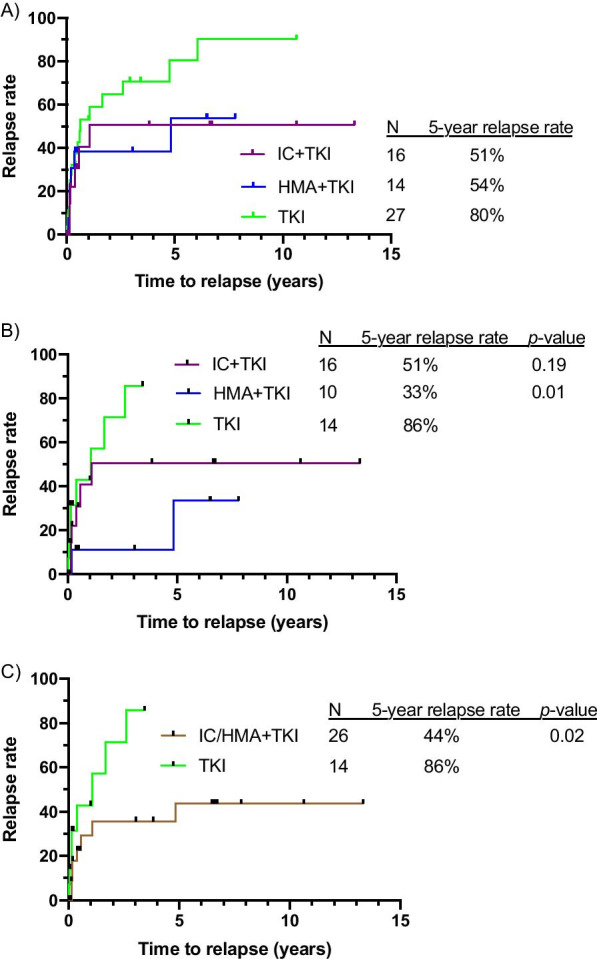
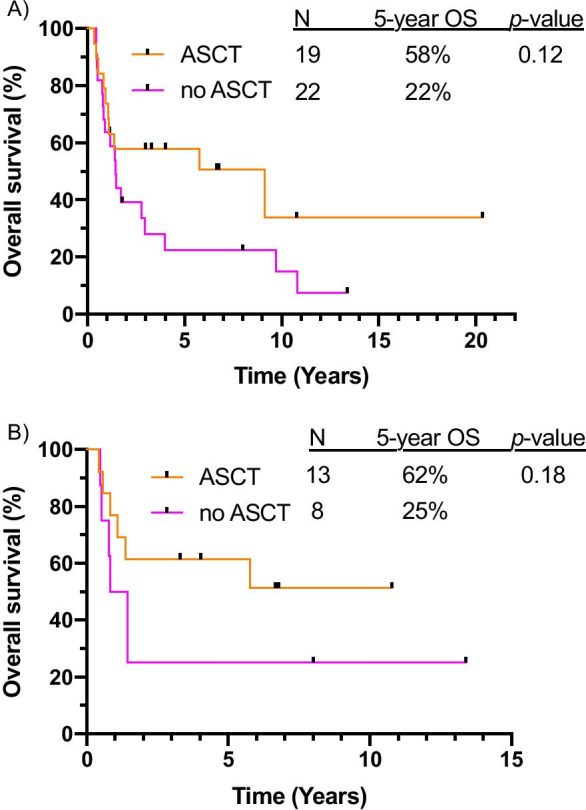
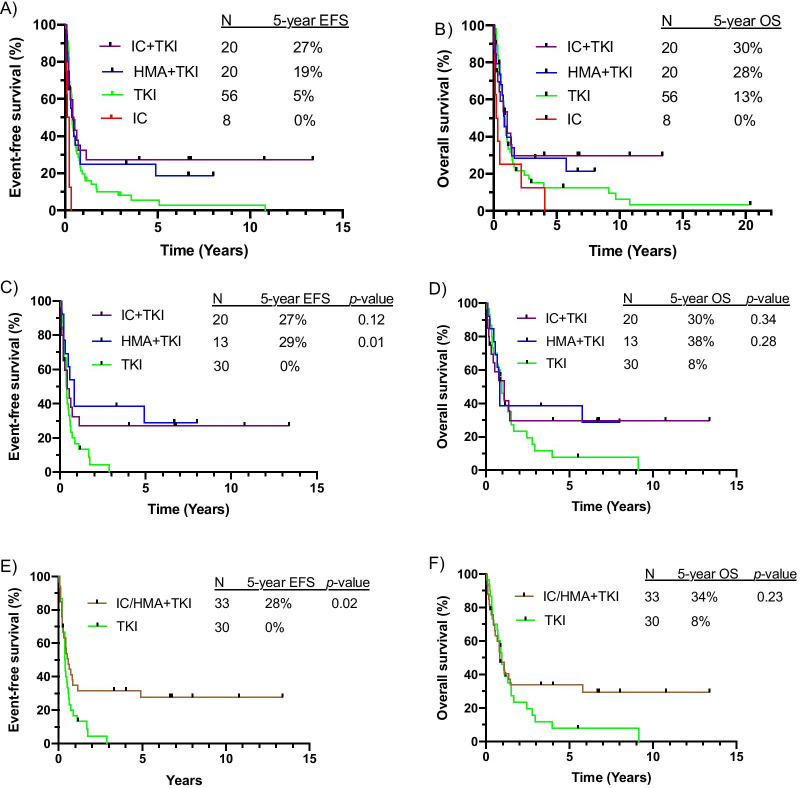
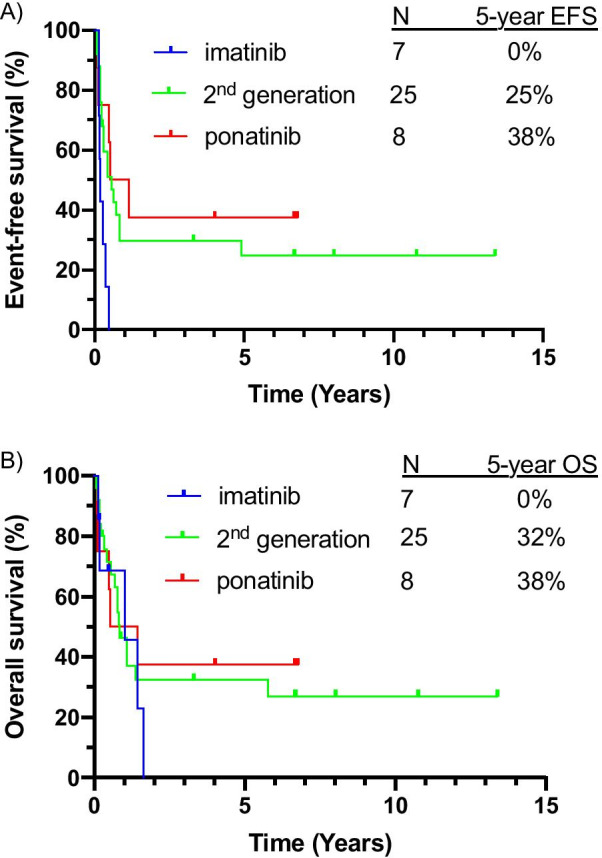
Response rates were similar between patients treated with IC + TKI and HMA + TKI. Compared to treatment with TKI alone, treatment with IC/HMA + TKI resulted in a higher rate of complete remission (CR) or CR with incomplete count recovery (CRi) (57.5% vs 33.9%, p < 0.05), a higher complete cytogenetic response rate (45% vs 10.7%, p < 0.001), and more patients proceeding to ASCT (32.5% vs 10.7%, p < 0.01). With a median follow-up of 6.7 years, long-term outcomes were similar between the IC + TKI and HMA + TKI groups. Combination therapy with IC/HMA + TKI was superior to therapy with TKI alone, including when analysis was limited to those treated with a 2nd/3rd-generation TKI. When using a 2nd/3rd-generation TKI, IC/HMA + TKI led to lower 5-year cumulative incidence of relapse (CIR; 44% vs 86%, p < 0.05) and superior 5-year event-free survival (EFS; 28% vs 0%, p < 0.05) and overall survival (OS; 34% vs 8%, p = 0.23) compared to TKI alone. Among patients who received IC/HMA + TKI, EFS and OS was superior for patients who received a 2nd/3rd generation TKI compared to those who received imatinib-based therapy. In a landmark analysis, 5-year OS was higher for patients who proceeded to ASCT (58% vs 22%, p = 0.12).
Compared to patients treated with TKI alone for CML-MBP, treatment with IC + TKI or HMA + TKI led to improved response rates, CIR, EFS, and OS, particularly for patients who received a 2nd/3rd-generation TKI. Combination therapy with IC + TKI or HMA + TKI, rather than a TKI alone, should be considered the optimal treatment strategy for patients with CML-MBP.
未经治疗的慢性髓性白血病(CML)的自然病程是进展为侵袭性的急变期。即使在当前BCR-ABL1酪氨酸激酶抑制剂(TKIs)的时代,CML急变期的治疗效果仍然很差,且没有达成共识的一线治疗方案。
我们回顾性分析了2000年至2019年期间连续治疗的104例髓系急变期CML(CML-MBP)患者的缓解率和生存结果,这些患者基于4种不同的一线治疗方法进行治疗:强化化疗(IC)+TKI(n = 20)、去甲基化药物(HMA)+TKI(n = 20)、单纯TKI(n = 56)或单纯IC(n = 8)。我们还评估了TKI选择和随后的异基因干细胞移植(ASCT)对患者预后的影响。
接受IC + TKI和HMA + TKI治疗的患者之间的缓解率相似。与单纯TKI治疗相比,IC/HMA + TKI治疗导致更高的完全缓解(CR)或血细胞计数未完全恢复的CR(CRi)率(57.5%对33.9%,p < 0.05)、更高的完全细胞遗传学缓解率(45%对10.7%,p < 0.001),以及更多患者进行ASCT(32.5%对10.7%,p < 0.01)。中位随访6.7年,IC + TKI组和HMA + TKI组的长期结果相似。IC/HMA + TKI联合治疗优于单纯TKI治疗,包括当分析仅限于接受第二代/第三代TKI治疗的患者时。当使用第二代/第三代TKI时,与单纯TKI相比,IC/HMA + TKI导致更低的5年累积复发率(CIR;44%对86%,p < 0.05)和更好的5年无事件生存率(EFS;28%对0%)以及总生存率(OS;34%对8%,p = 0.23)。在接受IC/HMA + TKI治疗的患者中,接受第二代/第三代TKI治疗的患者的EFS和OS优于接受基于伊马替尼治疗的患者。在一项标志性分析中,进行ASCT的患者的5年OS更高(58%对22%,p = 0.12)。
与单纯TKI治疗CML-MBP的患者相比,IC + TKI或HMA + TKI治疗导致缓解率、CIR、EFS和OS得到改善,特别是对于接受第二代/第三代TKI治疗的患者。IC + TKI或HMA + TKI联合治疗,而不是单纯TKI,应被视为CML-MBP患者的最佳治疗策略。