Department of Medical Oncology, IRCCS Istituto Romagnolo per lo Studio dei Tumori 'Dino Amadori'-IRST, Meldola, Italy.
Division of Gastroenterology, Department of Medicine, Kurume University School of Medicine, Kurume, Japan.
ESMO Open. 2021 Aug;6(4):100190. doi: 10.1016/j.esmoop.2021.100190. Epub 2021 Jun 16.
After the advent of new treatment options for advanced hepatocellular carcinoma (HCC), the identification of prognostic factors is crucial for the selection of the most appropriate therapy for each patient.
With the aim to fill this gap, we applied recursive partitioning analysis (RPA) to a cohort of 404 patients treated with lenvatinib.
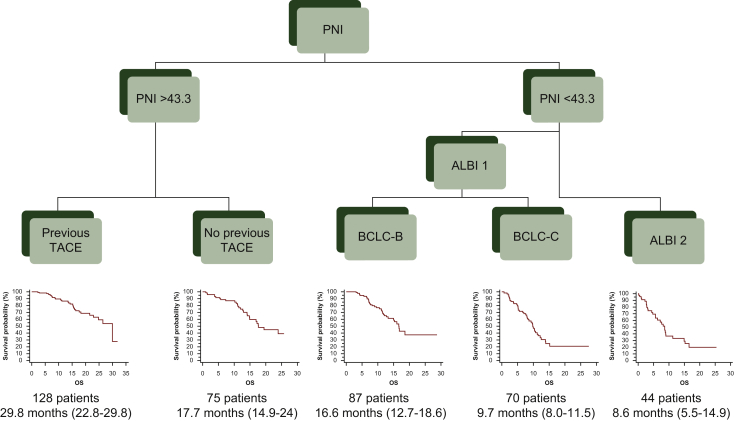
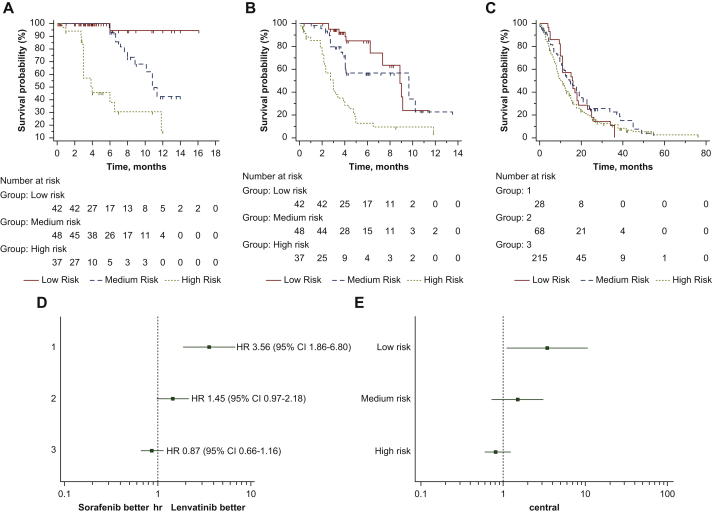
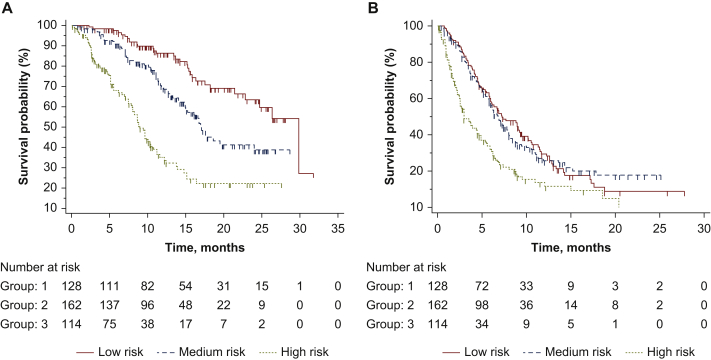
The application of RPA resulted in a classification based on five variables that originated a new prognostic score, the lenvatinib prognostic index (LEP) index, identifying three groups: low risk [patients with prognostic nutritional index (PNI) >43.3 and previous trans-arterial chemoembolization (TACE)]; medium risk [patients with PNI >43.3 but without previous TACE and patients with PNI <43.3, albumin-bilirubin (ALBI) grade 1 and Barcelona Clinic Liver Cancer stage B (BCLC-B)]; high risk [patients with PNI <43.3 and ALBI grade 2 and patients with PNI <43.3, albumin-bilirubin (ALBI) grade 1 and Barcelona Clinic Liver Cancer stage C (BCLC-C)]. Median overall survival was 29.8 months [95% confidence interval (CI) 22.8-29.8 months] in low risk patients (n = 128), 17.0 months (95% CI 15.0-24.0 months) in medium risk (n = 162) and 8.9 months (95% CI 8.0-10.7 months) in high risk (n = 114); low risk hazard ratio (HR) 1 (reference group), medium risk HR 1.95 (95% CI 1.38-2.74), high risk HR 4.84 (95% CI 3.16-7.43); P < 0.0001. The LEP index was validated in a cohort of 127 Italian patients treated with lenvatinib. While the same classification did not show a prognostic value in a cohort of 311 patients treated with sorafenib, we also show a possible predictive role in favor of lenvatinib in the low risk group.
LEP index is a promising, easy-to-use tool that may be used to stratify patients undergoing systemic treatment of advanced HCC.
新的治疗方案问世后,晚期肝细胞癌(HCC)的预后因素分析对于为每位患者选择最合适的治疗方案至关重要。
为填补这一空白,我们对接受乐伐替尼治疗的 404 例患者进行了递归分区分析(RPA)。
RPA 应用产生了基于 5 个变量的分类,从而产生了新的预后评分——乐伐替尼预后指数(LEP)指数,将患者分为 3 组:低危组[预后营养指数(PNI)>43.3 且既往接受过经动脉化疗栓塞术(TACE)];中危组[PNI>43.3 但未接受 TACE 治疗,以及 PNI<43.3、白蛋白-胆红素(ALBI)分级 1 和巴塞罗那临床肝癌分期 B(BCLC-B)];高危组[PNI<43.3 且 ALBI 分级 2 和 PNI<43.3,ALBI 分级 1 和巴塞罗那临床肝癌分期 C(BCLC-C)]。低危组患者中位总生存期为 29.8 个月[95%置信区间(CI)22.8-29.8 个月](n=128),中危组为 17.0 个月(95%CI 15.0-24.0 个月)(n=162),高危组为 8.9 个月(95%CI 8.0-10.7 个月)(n=114);低危组风险比(HR)为 1(参考组),中危组 HR 为 1.95(95%CI 1.38-2.74),高危组 HR 为 4.84(95%CI 3.16-7.43);P<0.0001。该 LEP 指数在接受乐伐替尼治疗的 127 名意大利患者队列中得到验证。虽然同样的分类在接受索拉非尼治疗的 311 名患者队列中没有显示出预后价值,但我们也显示了 LEP 指数在低危组中可能具有预测作用。
LEP 指数是一种有前途的、易于使用的工具,可用于对接受晚期 HCC 系统治疗的患者进行分层。