Menon Jagadeesh, Vij Mukul, Sachan Deepti, Rammohan Ashwin, Shanmugam Naresh, Kaliamoorthy Ilankumaran, Rela Mohamed
Institute of Liver Disease and Transplantation, Dr Rela Institute and Medical Center, Chennai 600044, Tamil Nadu, India.
Department of Pathology, Dr Rela Institute and Medical Center, Chennai 600044, Tamil Nadu, India.
World J Transplant. 2021 Jun 18;11(6):161-179. doi: 10.5500/wjt.v11.i6.161.
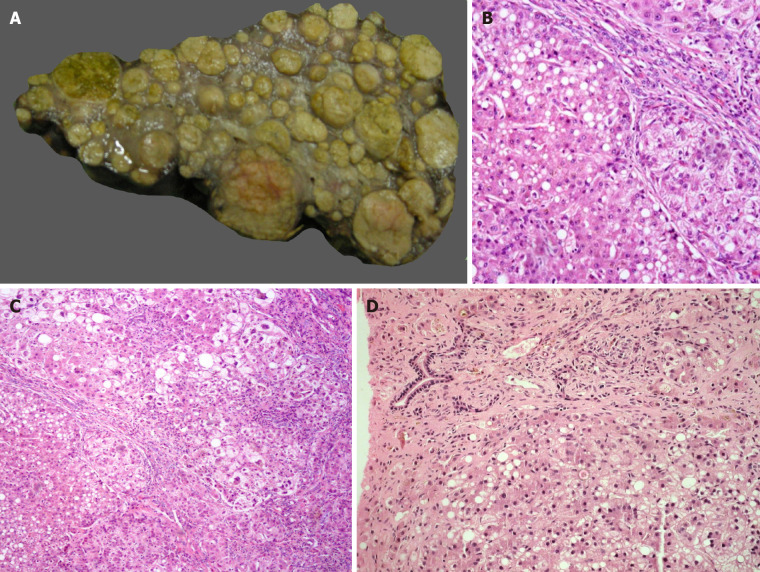
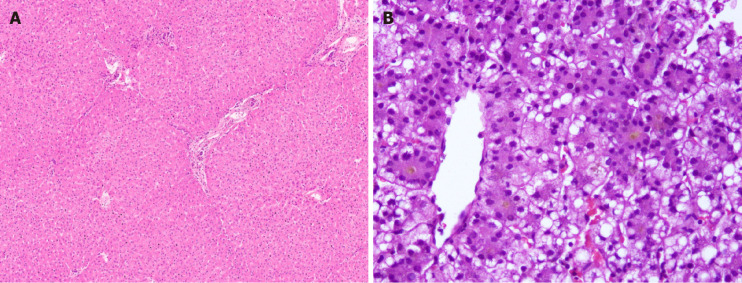
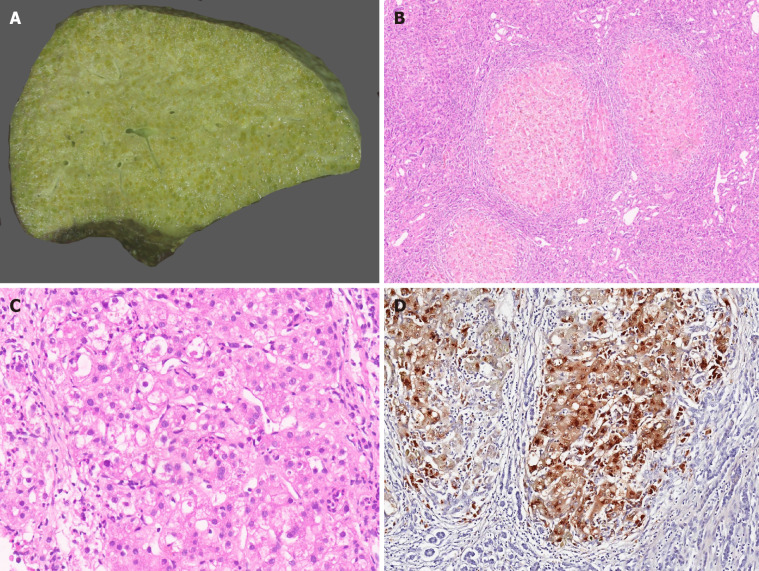
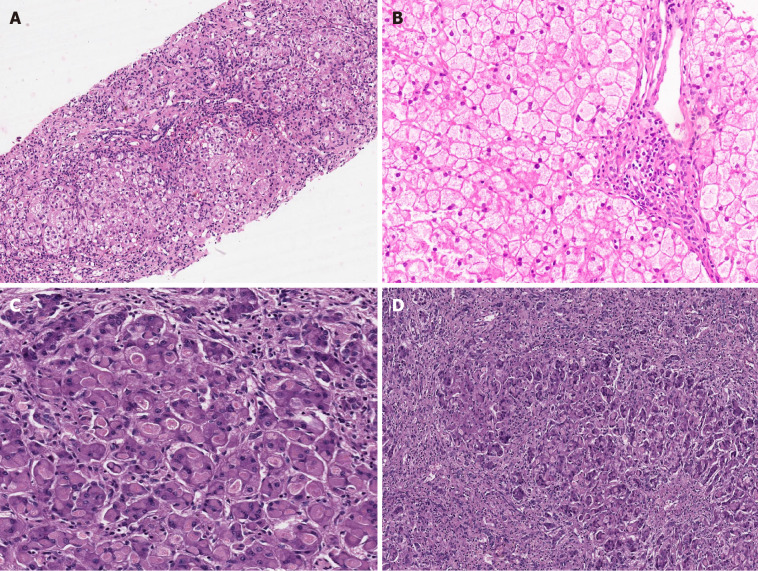
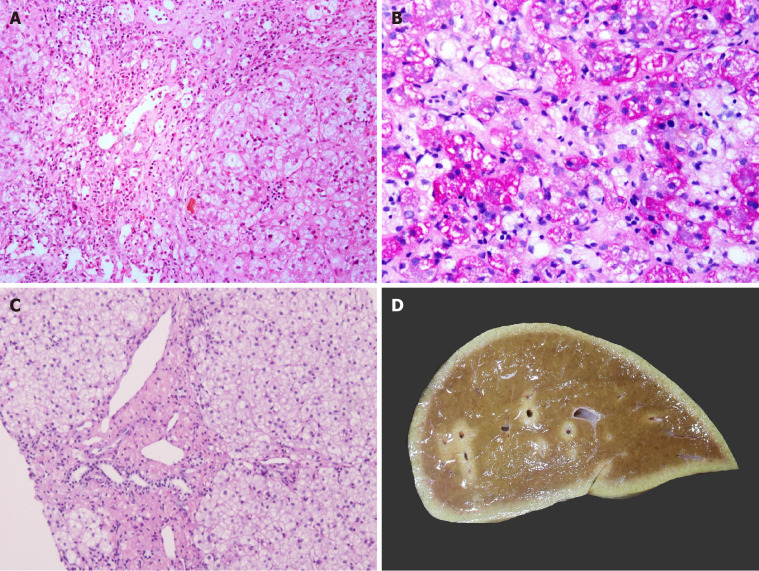
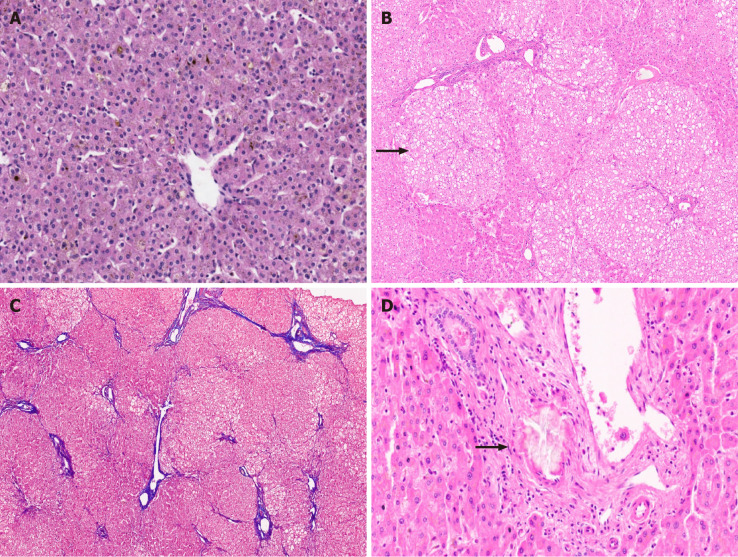
Metabolic liver diseases (MLD) are the second most common indication for liver transplantation (LT) in children. This is based on the fact that the majority of enzymes involved in various metabolic pathways are present within the liver and LT can cure or at least control the disease manifestation. LT is also performed in metabolic disorders for end-stage liver disease, its sequelae including hepatocellular cancer. It is also performed for preventing metabolic crisis', arresting progression of neurological dysfunction with a potential to reverse symptoms in some cases and for preventing damage to end organs like kidneys as in the case of primary hyperoxalosis and methyl malonic acidemia. Pathological findings in explant liver with patients with metabolic disease include unremarkable liver to steatosis, cholestasis, inflammation, variable amount of fibrosis, and cirrhosis. The outcome of LT in metabolic disorders is excellent except for patients with mitochondrial disorders where significant extrahepatic involvement leads to poor outcomes and hence considered a contraindication for LT. A major advantage of LT is that in the post-operative period most patients can discontinue the special formula which they were having prior to the transplant and this increases their well-being and improves growth parameters. Auxiliary partial orthotopic LT has been described for patients with noncirrhotic MLD where a segmental graft is implanted in an orthotopic position after partial resection of the native liver. The retained native liver can be the potential target for future gene therapy when it becomes a clinical reality.
代谢性肝病(MLD)是儿童肝移植(LT)的第二大常见适应症。这是基于以下事实:参与各种代谢途径的大多数酶都存在于肝脏中,肝移植可以治愈或至少控制疾病表现。肝移植也用于治疗终末期肝病及其后遗症(包括肝细胞癌)的代谢紊乱。它还用于预防“代谢危机”,阻止神经功能障碍的进展,在某些情况下有可能逆转症状,并用于预防像原发性高草酸尿症和甲基丙二酸血症患者那样对肾脏等终末器官的损害。代谢性疾病患者的移植肝病理表现包括从无明显异常到脂肪变性、胆汁淤积、炎症、不同程度的纤维化和肝硬化。除了线粒体疾病患者外,代谢紊乱患者肝移植的效果都很好,线粒体疾病患者存在明显的肝外受累,导致预后不良,因此被认为是肝移植的禁忌症。肝移植的一个主要优点是,在术后大多数患者可以停用移植前使用的特殊配方奶粉,这提高了他们的生活质量并改善了生长指标。对于非肝硬化性代谢性肝病患者,已描述了辅助性部分原位肝移植,即在部分切除自身肝脏后,将节段性移植物原位植入。当未来基因治疗成为临床现实时,保留的自身肝脏可能成为其潜在靶点。