Department of Reproductive Medical Center, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, China.
Reproductive Medicine Center, Tongji Medical College, Huazhong University of Science and Technology, Wuhan Tongji Reproductive Medicine Hospital, Wuhan, Hubei, China.
J Clin Lab Anal. 2021 Aug;35(8):e23882. doi: 10.1002/jcla.23882. Epub 2021 Jun 28.
In this study, we investigated the clinical value of serum Inhibin B alone or in combination with other hormone indicators in subfertile men.
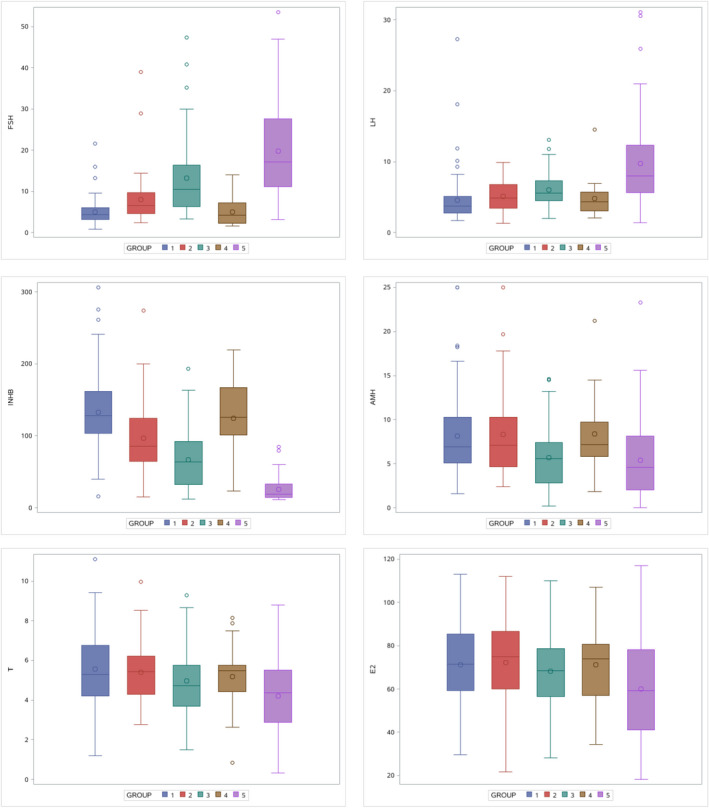
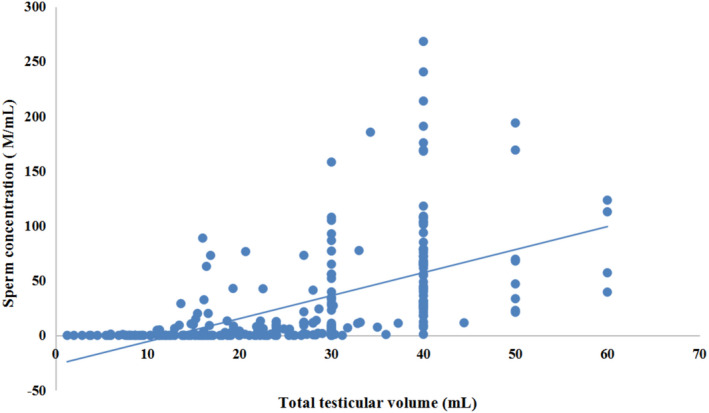
This is a multicenter study involving 324 men from different cities in China. Testicular volume, routine semen analysis, serum Inhibin B, anti-Müllerian hormone (AMH), follicle-stimulating hormone (FSH), luteinizing hormone (LH), testosterone, estradiol, and prolactin were measured. Testicular tissue samples were also analyzed in 78 of 129 patients with azoospermia to distinguish impaired spermatogenesis from obstructive azoospermia.
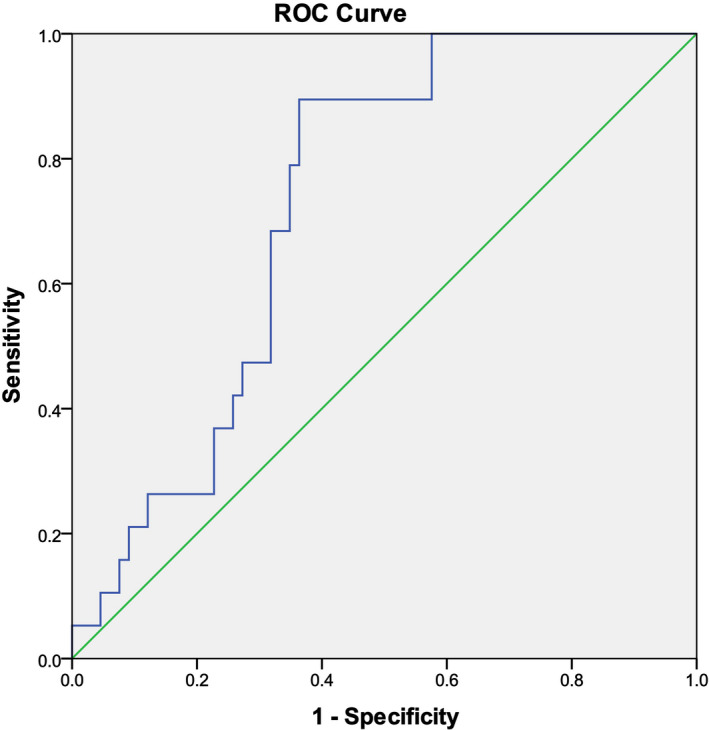
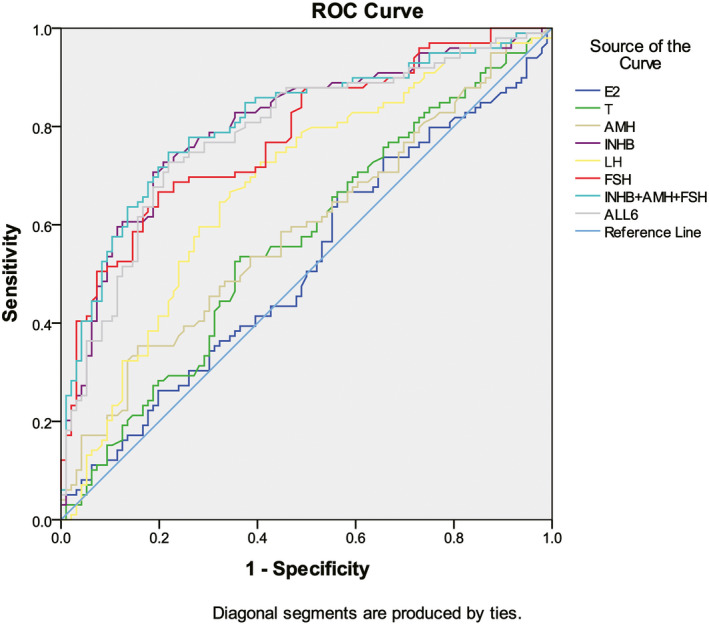
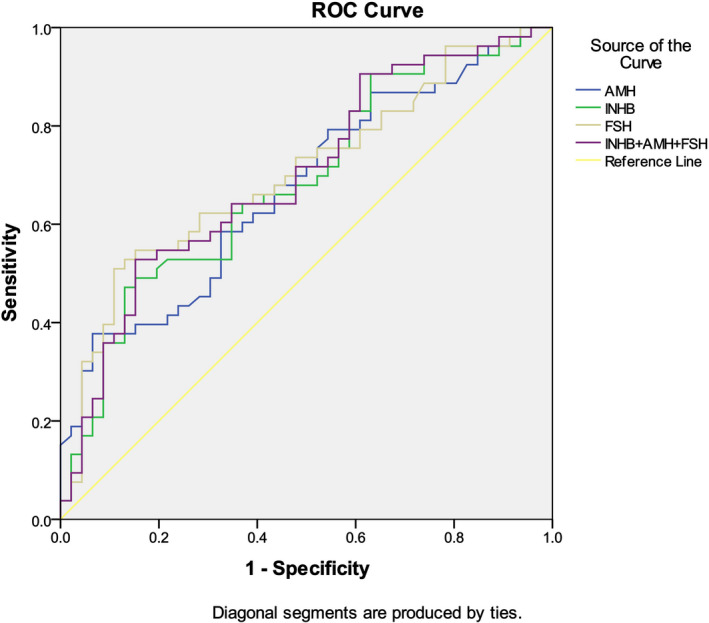
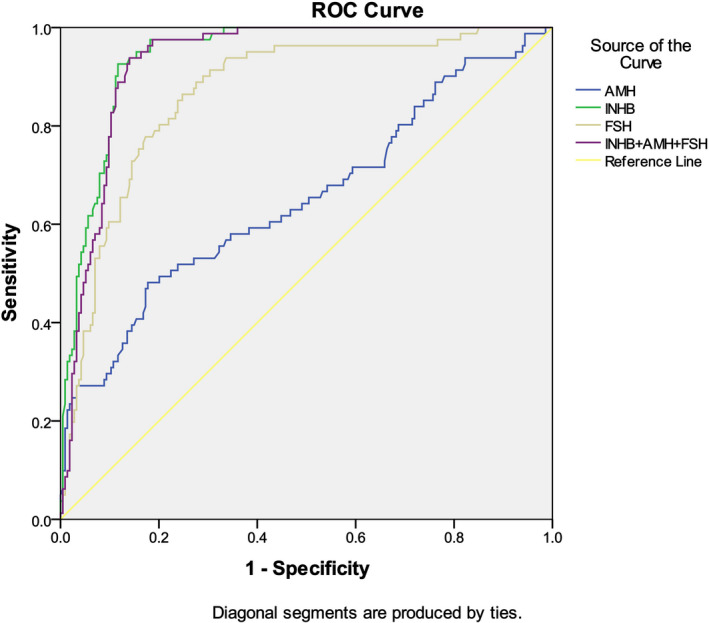
The concentration of Inhibin B, FSH, and AMH is related to spermatogenesis. For men with impaired spermatogenesis, including mild-to-moderate oligozoospermia (IMO) and severe oligozoospermia (ISO), serum levels of Inhibin B and FSH are highly correlated with sperm counting. However, in patients with idiopathic moderate oligozoospermia or severe oligozoospermia, there was no significant correlation between Inhibin B (or FSH) and sperm concentration. The upper cutoff value of Inhibin B to diagnose ISO is 58.25 pg/ml with a predictive accuracy of 80.65%. To distinguish between nonobstructive azoospermia (NOA) and obstructive azoospermia (OA), the area under the curve (AUC) for AMH + Inhibin B + FSH is very similar to Inhibin B (0.943 vs. 0.941). The cutoff level of Inhibin B to diagnose nonobstructive azoospermia is 45.9 pg/ml with a positive and negative prediction accuracy of 97.70% and 85.71%, respectively.
In summary, Inhibin B is a promising biomarker alone or in combination with other hormone indicators for the diagnosis of testicular spermatogenesis status, helping clinical doctors to distinguish NOA from OA.
本研究旨在探讨血清抑制素 B 单独或联合其他激素指标在男性不育症中的临床价值。
这是一项多中心研究,共纳入来自中国不同城市的 324 名男性。检测睾丸体积、常规精液分析、血清抑制素 B、抗苗勒管激素(AMH)、卵泡刺激素(FSH)、黄体生成素(LH)、睾酮、雌二醇和催乳素。还对 129 例无精子症患者中的 78 例进行了睾丸组织分析,以区分生精障碍型和梗阻型无精子症。
抑制素 B、FSH 和 AMH 的浓度与精子发生有关。对于生精障碍的男性,包括轻度至中度少精子症(IMO)和重度少精子症(ISO),血清抑制素 B 和 FSH 水平与精子计数高度相关。然而,在特发性中度少精子症或重度少精子症患者中,抑制素 B(或 FSH)与精子浓度之间无显著相关性。诊断 ISO 的抑制素 B 上限值为 58.25 pg/ml,预测准确率为 80.65%。为了区分非梗阻性无精子症(NOA)和梗阻性无精子症(OA),AMH+抑制素 B+FSH 的曲线下面积(AUC)与抑制素 B 非常相似(0.943 对 0.941)。诊断非梗阻性无精子症的抑制素 B 截断值为 45.9 pg/ml,阳性和阴性预测准确率分别为 97.70%和 85.71%。
综上所述,抑制素 B 是一种很有前途的生物标志物,可单独或联合其他激素指标用于诊断睾丸生精状态,有助于临床医生区分 NOA 和 OA。