Centre for Public Health Kinetics (CPHK), New Delhi, Delhi, India.
Centre of Excellence in Women and Child Health, The Aga Khan University, Karachi, Pakistan.
PLoS Med. 2021 Jun 28;18(6):e1003644. doi: 10.1371/journal.pmed.1003644. eCollection 2021 Jun.
Maternal morbidity occurs several times more frequently than mortality, yet data on morbidity burden and its effect on maternal, foetal, and newborn outcomes are limited in low- and middle-income countries. We aimed to generate prospective, reliable population-based data on the burden of major direct maternal morbidities in the antenatal, intrapartum, and postnatal periods and its association with maternal, foetal, and neonatal death in South Asia and sub-Saharan Africa.
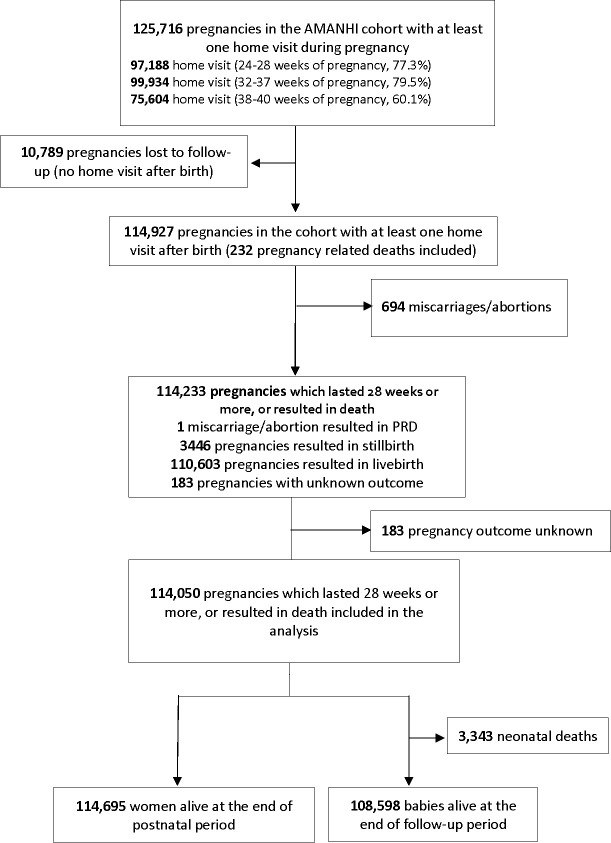
This is a prospective cohort study, conducted in 9 research sites in 8 countries of South Asia and sub-Saharan Africa. We conducted population-based surveillance of women of reproductive age (15 to 49 years) to identify pregnancies. Pregnant women who gave consent were include in the study and followed up to birth and 42 days postpartum from 2012 to 2015. We used standard operating procedures, data collection tools, and training to harmonise study implementation across sites. Three home visits during pregnancy and 2 home visits after birth were conducted to collect maternal morbidity information and maternal, foetal, and newborn outcomes. We measured blood pressure and proteinuria to define hypertensive disorders of pregnancy and woman's self-report to identify obstetric haemorrhage, pregnancy-related infection, and prolonged or obstructed labour. Enrolled women whose pregnancy lasted at least 28 weeks or those who died during pregnancy were included in the analysis. We used meta-analysis to combine site-specific estimates of burden, and regression analysis combining all data from all sites to examine associations between the maternal morbidities and adverse outcomes. Among approximately 735,000 women of reproductive age in the study population, and 133,238 pregnancies during the study period, only 1.6% refused consent. Of these, 114,927 pregnancies had morbidity data collected at least once in both antenatal and in postnatal period, and 114,050 of them were included in the analysis. Overall, 32.7% of included pregnancies had at least one major direct maternal morbidity; South Asia had almost double the burden compared to sub-Saharan Africa (43.9%, 95% CI 27.8% to 60.0% in South Asia; 23.7%, 95% CI 19.8% to 27.6% in sub-Saharan Africa). Antepartum haemorrhage was reported in 2.2% (95% CI 1.5% to 2.9%) pregnancies and severe postpartum in 1.7% (95% CI 1.2% to 2.2%) pregnancies. Preeclampsia or eclampsia was reported in 1.4% (95% CI 0.9% to 2.0%) pregnancies, and gestational hypertension alone was reported in 7.4% (95% CI 4.6% to 10.1%) pregnancies. Prolonged or obstructed labour was reported in about 11.1% (95% CI 5.4% to 16.8%) pregnancies. Clinical features of late third trimester antepartum infection were present in 9.1% (95% CI 5.6% to 12.6%) pregnancies and those of postpartum infection in 8.6% (95% CI 4.4% to 12.8%) pregnancies. There were 187 pregnancy-related deaths per 100,000 births, 27 stillbirths per 1,000 births, and 28 neonatal deaths per 1,000 live births with variation by country and region. Direct maternal morbidities were associated with each of these outcomes.
Our findings imply that health programmes in sub-Saharan Africa and South Asia must intensify their efforts to identify and treat maternal morbidities, which affected about one-third of all pregnancies and to prevent associated maternal and neonatal deaths and stillbirths.
The study is not a clinical trial.
产妇发病率比死亡率高好几倍,但在中低收入国家,发病率负担及其对产妇、胎儿和新生儿结局的影响的数据有限。我们旨在生成前瞻性的、可靠的基于人群的主要直接产妇发病率的负担数据,这些发病率发生在产前、产时和产后期间,并将其与南亚和撒哈拉以南非洲的产妇、胎儿和新生儿死亡相关联。
这是一项前瞻性队列研究,在南亚和撒哈拉以南非洲的 8 个国家的 9 个研究地点进行。我们进行了基于人群的育龄妇女(15 至 49 岁)监测,以确定妊娠情况。同意参与研究的孕妇被纳入研究,并随访至分娩和产后 42 天,时间从 2012 年至 2015 年。我们使用标准操作程序、数据收集工具和培训,以协调各地点的研究实施。在怀孕期间进行 3 次家访,在产后进行 2 次家访,以收集产妇发病率信息和产妇、胎儿和新生儿结局。我们测量血压和蛋白尿来定义妊娠高血压疾病,并通过妇女的自我报告来确定产科出血、妊娠相关感染和产程延长或梗阻。至少妊娠 28 周或在妊娠期间死亡的孕妇被纳入分析。我们使用荟萃分析来结合特定地点的发病率负担估计值,以及使用结合所有地点的所有数据的回归分析来检查产妇发病率与不良结局之间的关联。在研究人群中约有 735,000 名育龄妇女和 133,238 次妊娠期间,只有 1.6%的人拒绝同意。其中,114,927 次妊娠在产前和产后期间至少有一次收集了发病率数据,其中 114,050 次妊娠被纳入分析。总体而言,32.7%的纳入妊娠存在至少一种主要的直接产妇发病率;与撒哈拉以南非洲相比,南亚的发病率负担几乎是后者的两倍(43.9%,95%CI 27.8%至 60.0%在南亚;23.7%,95%CI 19.8%至 27.6%在撒哈拉以南非洲)。2.2%(95%CI 1.5%至 2.9%)的妊娠报告有产前出血,1.7%(95%CI 1.2%至 2.2%)的妊娠报告有严重产后出血。1.4%(95%CI 0.9%至 2.0%)的妊娠报告有子痫前期或子痫,7.4%(95%CI 4.6%至 10.1%)的妊娠报告有单纯性妊娠高血压。约 11.1%(95%CI 5.4%至 16.8%)的妊娠报告有产程延长或梗阻。晚期第三孕期产前感染的临床特征出现在 9.1%(95%CI 5.6%至 12.6%)的妊娠中,产后感染的临床特征出现在 8.6%(95%CI 4.4%至 12.8%)的妊娠中。每 100,000 次分娩中有 187 例妊娠相关死亡,每 1,000 次分娩中有 27 例死产,每 1,000 例活产中有 28 例新生儿死亡,这些数据因国家和地区而异。直接产妇发病率与这些结局均相关。
我们的研究结果表明,撒哈拉以南非洲和南亚的卫生规划必须加紧努力,以识别和治疗发病率约占所有妊娠三分之一的产妇发病率,并预防相关的产妇和新生儿死亡和死产。
该研究不是临床试验。