University College London, London, United Kingdom.
London School of Hygiene &Tropical Medicine, London, United Kingdom.
PLoS Med. 2021 Jun 29;18(6):e1003672. doi: 10.1371/journal.pmed.1003672. eCollection 2021 Jun.
Type 2 diabetes is 2-3 times more prevalent in people of South Asian and African/African Caribbean ethnicity than people of European ethnicity living in the UK. The former 2 groups also experience excess atherosclerotic cardiovascular disease (ASCVD) complications of diabetes. We aimed to study ethnic differences in statin initiation, a cornerstone of ASCVD primary prevention, for people with type 2 diabetes.
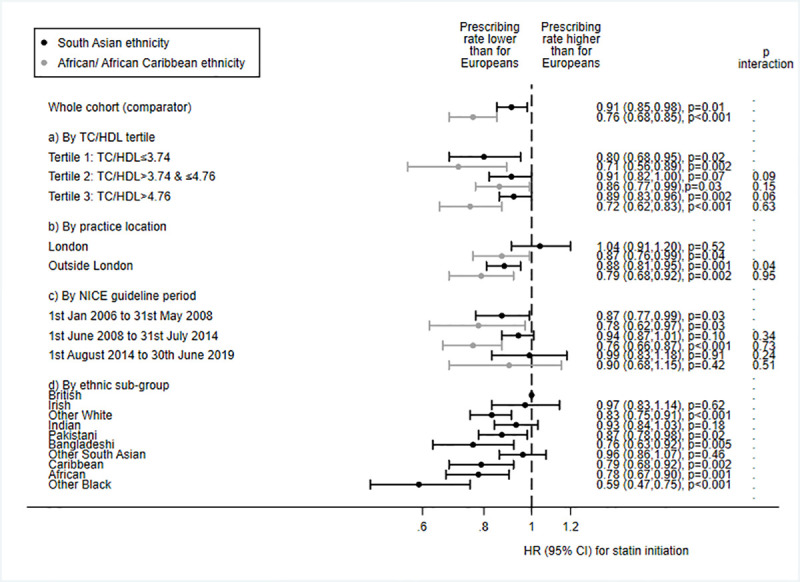
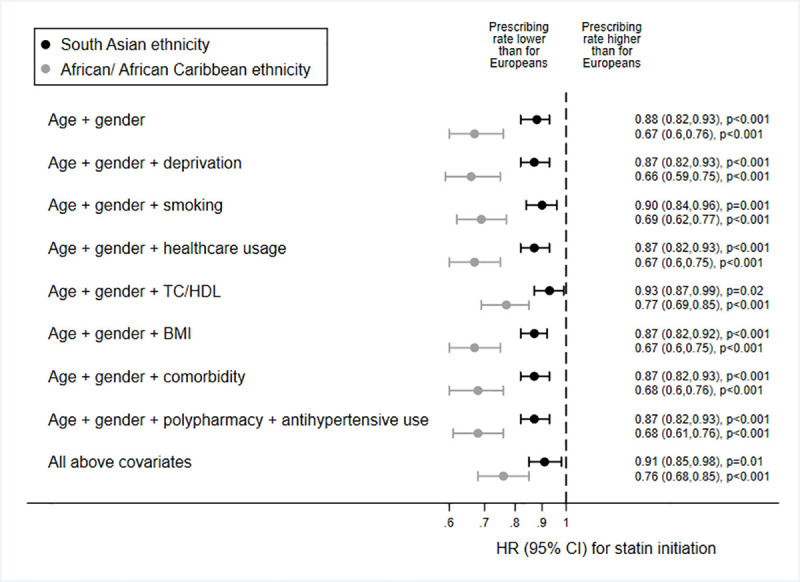
Observational cohort study of UK primary care records, from 1 January 2006 to 30 June 2019. Data were studied from 27,511 (88%) people of European ethnicity, 2,386 (8%) people of South Asian ethnicity, and 1,142 (4%) people of African/African Caribbean ethnicity with incident type 2 diabetes, no previous ASCVD, and statin use indicated by guidelines. Statin initiation rates were contrasted by ethnicity, and the number of ASCVD events that could be prevented by equalising prescribing rates across ethnic groups was estimated. Median time to statin initiation was 79, 109, and 84 days for people of European, South Asian, and African/African Caribbean ethnicity, respectively. People of African/African Caribbean ethnicity were a third less likely to receive guideline-indicated statins than European people (n/N [%]: 605/1,142 [53%] and 18,803/27,511 [68%], respectively; age- and gender-adjusted HR 0.67 [95% CI 0.60 to 0.76], p < 0.001). The HR attenuated marginally in a model adjusting for total cholesterol/high-density lipoprotein cholesterol ratio (0.77 [95% CI 0.69 to 0.85], p < 0.001), with no further diminution when deprivation, ASCVD risk factors, comorbidity, polypharmacy, and healthcare usage were accounted for (fully adjusted HR 0.76 [95% CI 0.68, 0.85], p < 0.001). People of South Asian ethnicity were 10% less likely to receive a statin than European people (1,489/2,386 [62%] and 18,803/27,511 [68%], respectively; fully adjusted HR 0.91 [95% CI 0.85 to 0.98], p = 0.008, adjusting for all covariates). We estimated that up to 12,600 ASCVD events could be prevented over the lifetimes of people currently affected by type 2 diabetes in the UK by equalising statin prescribing across ethnic groups. Limitations included incompleteness of recording of routinely collected data.
In this study we observed that people of African/African Caribbean ethnicity with type 2 diabetes were substantially less likely, and people of South Asian ethnicity marginally less likely, to receive guideline-indicated statins than people of European ethnicity, even after accounting for sociodemographics, healthcare usage, ASCVD risk factors, and comorbidity. Underuse of statins in people of African/African Caribbean or South Asian ethnicity with type 2 diabetes is a missed opportunity to prevent cardiovascular events.
在英国,南亚和非裔/加勒比裔人群患 2 型糖尿病的比例比欧洲裔人群高 2-3 倍,他们患糖尿病相关动脉粥样硬化性心血管疾病(ASCVD)并发症的风险也更高。我们旨在研究 2 型糖尿病患者起始他汀类药物治疗的种族差异,这是 ASCVD 一级预防的基石。
这是一项观察性队列研究,纳入了 2006 年 1 月 1 日至 2019 年 6 月 30 日期间英国初级保健记录中的数据。研究对象为 27511 名(88%)欧洲裔、2386 名(8%)南亚裔和 1142 名(4%)非裔/非裔加勒比裔 2 型糖尿病患者,这些患者无 ASCVD 病史且符合指南建议使用他汀类药物。按种族对比了起始他汀类药物治疗的情况,并估计了通过在不同种族群体中平等开具处方来预防多少 ASCVD 事件。欧洲、南亚和非裔/非裔加勒比裔人群起始他汀类药物治疗的中位时间分别为 79、109 和 84 天。与欧洲人相比,非裔/非裔加勒比裔人群接受指南推荐的他汀类药物治疗的可能性低三分之一(n/N[%]:1142/1142[53%]和 27511/27511[68%];年龄和性别调整后的 HR 0.67[95%CI 0.60 至 0.76],p<0.001)。在调整总胆固醇/高密度脂蛋白胆固醇比值的模型中,HR 略有减弱(0.77[95%CI 0.69 至 0.85],p<0.001),当调整贫困程度、ASCVD 风险因素、合并症、多种药物治疗和医疗保健使用情况后,HR 无进一步下降(完全调整后的 HR 0.76[95%CI 0.68 至 0.85],p<0.001)。与欧洲人相比,南亚裔人群接受他汀类药物治疗的可能性低 10%(1489/2386[62%]和 27511/27511[68%];完全调整后的 HR 0.91[95%CI 0.85 至 0.98],p=0.008,所有混杂因素调整后)。我们估计,通过在不同种族群体中平等开具他汀类药物处方,目前在英国受 2 型糖尿病影响的人群一生中可以预防多达 12600 例 ASCVD 事件。局限性包括常规收集数据的不完整性。
在这项研究中,我们观察到,与欧洲裔人群相比,非裔/非裔加勒比裔人群中 2 型糖尿病患者起始他汀类药物治疗的可能性明显较低,而南亚裔人群的可能性略低,即使考虑到社会人口统计学、医疗保健使用、ASCVD 风险因素和合并症。非裔/非裔加勒比裔或南亚裔 2 型糖尿病患者他汀类药物的使用不足是预防心血管事件的一个错失的机会。