Karl Landsteiner University of Health Sciences, Krems, Austria.
Department of Neurosurgery, University Hospital St. Poelten, Dunant-Platz 1, 3100, St. Poelten, Austria.
BMC Cancer. 2021 Jun 29;21(1):754. doi: 10.1186/s12885-021-08515-y.
Corticosteroid therapy (CST) prior to biopsy may hinder histopathological diagnosis in primary central nervous system lymphoma (PCNSL). Therefore, preoperative CST in patients with suspected PCNSL should be avoided if clinically possible. The aim of this study was thus to analyze the difference in the rate of diagnostic surgeries in PCNSL patients with and without preoperative CST.
A multicenter retrospective study including all immunocompetent patients diagnosed with PCNSL between 1/2004 and 9/2018 at four neurosurgical centers in Austria was conducted and the results were compared to literature.
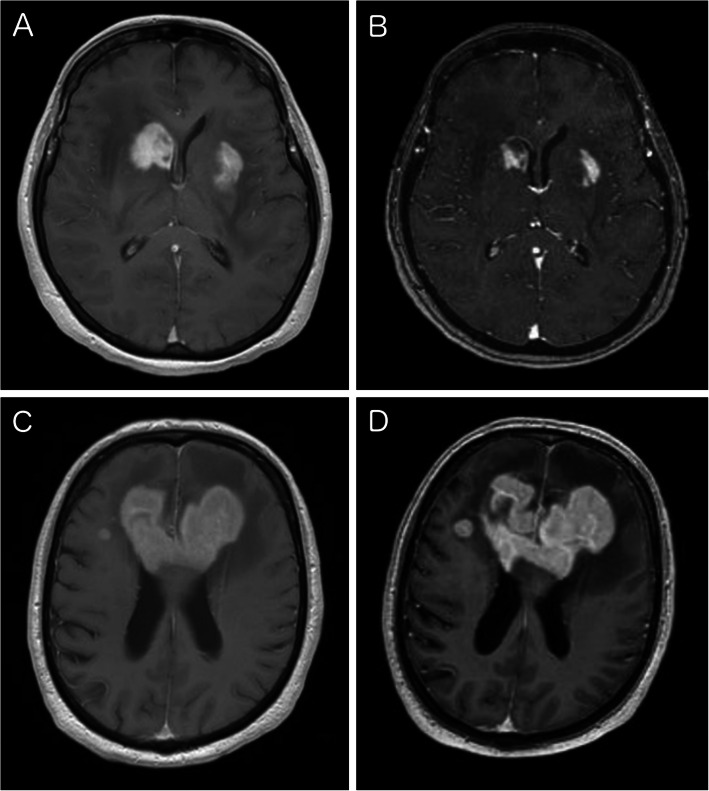
A total of 143 patients were included in this study. All patients showed visible contrast enhancement on preoperative MRI. There was no statistically significant difference in the rate of diagnostic surgeries with and without preoperative CST with 97.1% (68/70) and 97.3% (71/73), respectively (p = 1.0). Tapering and pause of CST did not influence the diagnostic rate. Including our study, there are 788 PCNSL patients described in literature with an odds ratio for inconclusive surgeries after CST of 3.3 (CI 1.7-6.4).
Preoperative CST should be avoided as it seems to diminish the diagnostic rate of biopsy in PCNSL patients. Yet, if CST has been administered preoperatively and there is still a contrast enhancing lesion to target for biopsy, surgeons should try to keep the diagnostic delay to a minimum as the likelihood for acquiring diagnostic tissue seems sufficiently high.
皮质类固醇治疗(CST)可能会阻碍原发性中枢神经系统淋巴瘤(PCNSL)的组织病理学诊断。因此,如果临床可行,应避免对疑似 PCNSL 患者进行术前 CST。本研究旨在分析 PCNSL 患者术前 CST 与无 CST 患者的诊断性手术率差异。
进行了一项多中心回顾性研究,纳入了 2004 年 1 月至 2018 年 9 月在奥地利四家神经外科中心诊断为 PCNSL 的所有免疫功能正常的患者,并将结果与文献进行了比较。
本研究共纳入 143 例患者。所有患者术前 MRI 均可见对比增强。有 CST 组和无 CST 组的诊断性手术率分别为 97.1%(68/70)和 97.3%(71/73),差异无统计学意义(p=1.0)。CST 的减量和暂停并未影响诊断率。包括本研究在内,文献中描述了 788 例 PCNSL 患者,CST 后手术结果不确定的比值比为 3.3(CI 1.7-6.4)。
术前 CST 应避免使用,因为它似乎会降低 PCNSL 患者活检的诊断率。然而,如果术前已给予 CST,并且仍有增强病变需要活检,外科医生应尽量将诊断延迟降至最低,因为获得诊断性组织的可能性似乎足够高。