Liao Chun-Kai, Lin Yueh-Chen, Hsu Yu-Jen, Chern Yih-Jong, You Jeng-Fu, Chiang Jy-Ming
Colorectal Section, Department of Surgery, Chang Gung Memorial Hospital, No. 5, Fuxing St., Guishan Dist,, Taoyuan, Taiwan, 33305.
College of Medicine, Chang Gung University, Taoyuan, Taiwan.
Hered Cancer Clin Pract. 2021 Jun 29;19(1):29. doi: 10.1186/s13053-021-00186-x.
Although extended colectomy (EC) was recommended for HNPCC patients, previous studies did not show significantly improved overall survival. Immunohistochemical (IHC) stain of mismatch repair (MMR) gene protein expression is now a feasible and reliable test clinically. Therefore, we tried to investigate whether we could use MMR IHC stain to select operation types in HNPCC patients.
Between 1995 and 2013, 186 HNPCC patients were collected. Status of MMR protein expression, perioperative clinic-pathological variables and post-operative follow up status were analyzed by multivariate analyses.
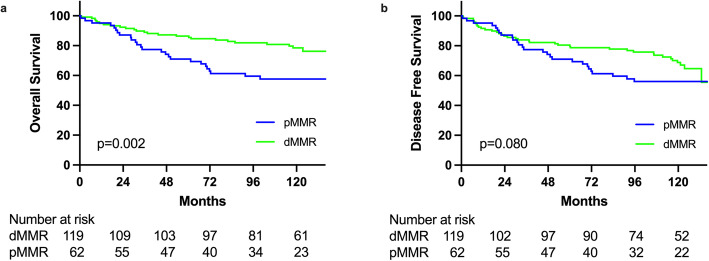
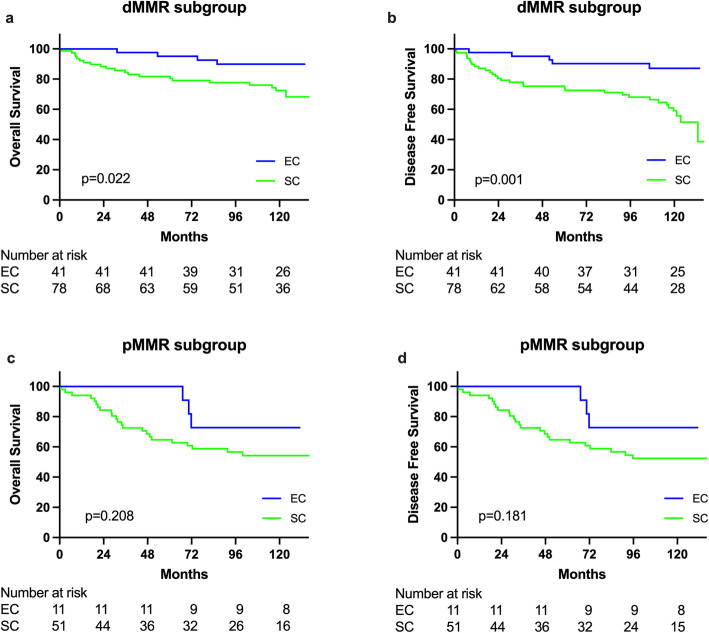
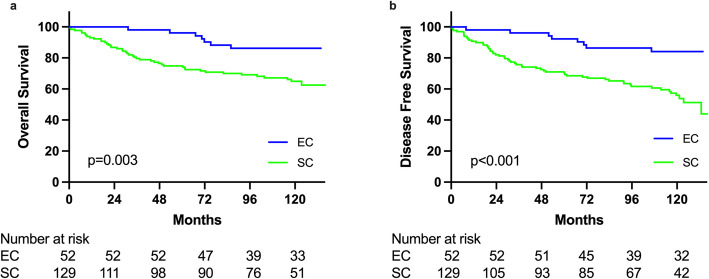
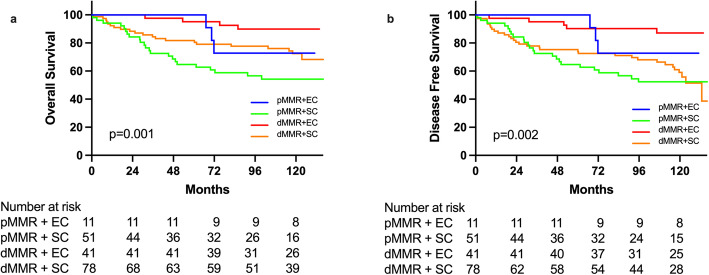
Sixty-five percent (121 of 186) patients of these HNPCC patients demonstrated loss of at least one MMR protein. There were several significant differences existing between deficient MMR (dMMR) and proficient MMR (pMMR) subgroups in terms of clinic-pathological characteristics. With the average follow-up duration of 93.9 months, we observed significantly high risk of developing metachronous CRC between SC and EC subgroups (crude rate 8.5% vs. 0%, p = 0.035). However, no significant difference was observed among the presence of extra-colonic tumors (12.4% vs. 5.8%, p = 0.284). The positive and negative prediction rate of metachronous CRC in dMMR subgroup was 12.8 and 87.2% while 1.9 and 98.1% in the pMMR subgroup. Survival outcomes were significantly affected by MMR status and resection types by multivariate analysis. Significantly better OS in dMMR subgroup (HR = 0.479, 95% CI: 0.257-0.894, p = 0.021) comparing with pMMR subgroup was observed. However, significant improved DFS (HR = 0.367, 95% CI: 0.172-.0787, p = 0.010) but not significant for OS (HR = 0.510, 95% CI: 0.219-1.150, p = 0.103) for EC subgroup compared with SC subgroup. Differences existing among different subgroups by combing extent of resection and MMR status. In dMMR subgroup, SC, compared with EC, demonstrated significantly worse DFS by multivariate analyses (HR = 3.526, 95% CI: 1.346-9.236, p = 0.010) but not for OS (HR = 2.387, 95% CI: 0.788-7.229, p = 0.124), however, no significantly differences of OS and DFS in pMMR subgroup between SC and EC were found.
Significantly better overall survival and higher rate of metachronous CRC exist in dMMR subgroup of HNPCC patients comparing with pMMR subgroup. Extended colectomy significantly improved DFS and was thus recommended for dMMR subgroup but not pMMR subgroup of HNPCC patients.
尽管推荐对遗传性非息肉病性结直肠癌(HNPCC)患者行扩大结肠切除术(EC),但既往研究未显示其总生存期有显著改善。错配修复(MMR)基因蛋白表达的免疫组织化学(IHC)染色目前在临床上是一种可行且可靠的检测方法。因此,我们试图研究是否可以使用MMR IHC染色来选择HNPCC患者的手术方式。
收集1995年至2013年间的186例HNPCC患者。通过多因素分析对MMR蛋白表达状态、围手术期临床病理变量及术后随访情况进行分析。
这些HNPCC患者中有65%(186例中的121例)至少有一种MMR蛋白表达缺失。在临床病理特征方面,错配修复缺陷(dMMR)亚组和错配修复正常(pMMR)亚组之间存在若干显著差异。平均随访时间为93.9个月,我们观察到单纯结肠切除术(SC)亚组和扩大结肠切除术(EC)亚组之间异时性结直肠癌发生风险显著较高(粗发生率8.5%对0%,p = 0.035)。然而,结肠外肿瘤的发生率在两组间无显著差异(12.4%对5.8%,p = 0.284)。dMMR亚组中异时性结直肠癌的阳性和阴性预测率分别为12.8%和87.2%,而pMMR亚组中分别为1.9%和98.1%。多因素分析显示,生存结局受MMR状态和切除类型的显著影响。与pMMR亚组相比,dMMR亚组的总生存期显著更好(风险比[HR]=0.479,95%可信区间[CI]:0.257 - 0.894,p = 0.021)。然而,与SC亚组相比,EC亚组的无病生存期显著改善(HR = 0.367,95% CI:0.172 - 0.787,p = 0.010),但总生存期无显著差异(HR = 0.510,95% CI:0.219 - 1.150,p = 0.103)。通过综合切除范围和MMR状态,不同亚组间存在差异。在dMMR亚组中,多因素分析显示SC组与EC组相比无病生存期显著更差(HR = 3.526,95% CI:1.346 - 9.236,p = 0.010),但总生存期无差异(HR = 2.387,95% CI:0.788 - 7.229,p = 0.124),然而,在pMMR亚组中,SC组和EC组之间的总生存期和无病生存期均无显著差异。
与pMMR亚组相比,HNPCC患者的dMMR亚组总生存期显著更好,异时性结直肠癌发生率更高。扩大结肠切除术显著改善了dMMR亚组的无病生存期,因此推荐用于HNPCC患者的dMMR亚组而非pMMR亚组。