Erenay Fatih Safa, Alagoz Oguzhan, Banerjee Ritesh, Said Adnan, Cima Robert R
Department of Management Sciences, University of Waterloo, Waterloo, Ontario, Canada.
Department of Industrial and Systems Engineering, University of Wisconsin-Madison, Madison, Wisconsin.
Cancer. 2016 Aug 15;122(16):2560-70. doi: 10.1002/cncr.30091. Epub 2016 Jun 1.
The incidence of metachronous colorectal cancer (MCRC) among colorectal cancer (CRC) survivors varies significantly, and the optimal colonoscopy surveillance practice for mitigating MCRC incidence is unknown.
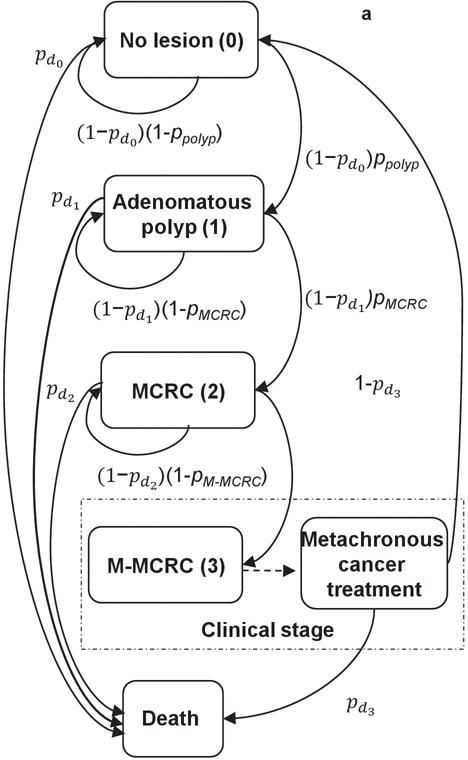
A cost-effectiveness analysis was used to compare the performances of the US Multi-Society Task Force guideline and all clinically reasonable colonoscopy surveillance strategies for 50- to 79-year-old posttreatment CRC patients with a computer simulation model.
The US guideline [(1,3,5)] recommends the first colonoscopy 1 year after treatment, whereas the second and third colonoscopies are to be repeated at 3- and 5-year intervals. Some promising alternative cost-effective strategies were identified. In comparison with the US guideline, under various scenarios for a 20-year period, 1) reducing the surveillance interval of the guideline after the first colonoscopy by 1 year [(1,2,5)] would save up to 78 discounted life-years (LYs) and prevent 23 MCRCs per 1000 patients (incremental cost-effectiveness ratio [ICER] ≤ $23,270/LY), 2) reducing the intervals after the first and second negative colonoscopies by 1 year [(1,2,4)] would save/prevent up to 109 discounted LYs and 36 MCRCs (ICER ≤ $52,155/LY), and 3) reducing the surveillance intervals after the first and second negative colonoscopy by 1 and 2 years [(1,2,3)] would save/prevent up to 141 discounted LYs and 50 MCRCs (ICER ≤ $63,822/LY). These strategies would require up to 1100 additional colonoscopies per 1000 patients. Although the US guideline might not be cost-effective in comparison with a less intensive oncology guideline [(3,3,5); the ICER could be as high as $140,000/LY], the promising strategies would be cost-effective in comparison with such less intensive guidelines unless the cumulative MCRC incidence were very low.
The US guideline might be improved by a slight increase in the surveillance intensity at the expense of moderately increased cost. More research is warranted to explore the benefits/harms of such practices. Cancer 2016;122:2560-70. © 2016 American Cancer Society.
结直肠癌(CRC)幸存者中异时性结直肠癌(MCRC)的发病率差异显著,而降低MCRC发病率的最佳结肠镜监测方案尚不清楚。
采用成本效益分析,通过计算机模拟模型比较美国多学会工作组指南和所有临床合理的结肠镜监测策略在50至79岁CRC治疗后患者中的表现。
美国指南[(1,3,5)]建议治疗后1年进行首次结肠镜检查,而第二次和第三次结肠镜检查应分别在3年和5年后重复进行。确定了一些有前景的替代成本效益策略。与美国指南相比,在20年的不同情况下,1)将首次结肠镜检查后指南的监测间隔缩短1年[(1,2,5)],每1000例患者最多可节省78个贴现生命年(LYs)并预防23例MCRC(增量成本效益比[ICER]≤23,270美元/LY),2)将首次和第二次结肠镜检查阴性后的间隔缩短1年[(1,2,4)],最多可节省/预防109个贴现LYs和36例MCRC(ICER≤52,155美元/LY),3)将首次和第二次结肠镜检查阴性后的监测间隔分别缩短1年和2年[(1,2,3)],最多可节省/预防141个贴现LYs和50例MCRC(ICER≤63,822美元/LY)。这些策略每1000例患者最多需要额外进行1100次结肠镜检查。尽管与强度较低的肿瘤学指南[(3,3,5)]相比,美国指南可能不具有成本效益(ICER可能高达140,000美元/LY),但除非MCRC的累积发病率非常低,否则这些有前景的策略与这种强度较低的指南相比将具有成本效益。
美国指南可能通过略微提高监测强度来改进,代价是成本适度增加。有必要进行更多研究以探索此类做法的益处/危害。《癌症》2016年;122:2560 - 70。©2016美国癌症协会。