Perfusion Department, Great Ormond Street Hospital, London, UK; Institute of Cardiovascular Science, University College London, London, UK; Digital Research Informatics and Virtual Environment Unit, NIHR Great Ormond Street Hospital BRC, London, UK.
Digital Research Informatics and Virtual Environment Unit, NIHR Great Ormond Street Hospital BRC, London, UK.
J Heart Lung Transplant. 2021 Nov;40(11):1433-1442. doi: 10.1016/j.healun.2021.05.010. Epub 2021 May 29.
Intraoperative anti-A/B immunoadsorption (ABO-IA) was recently introduced for ABO-incompatible heart transplantation. Here we report the first case series of patients transplanted with ABO-IA, and compare outcomes with those undergoing plasma exchange facilitated ABO-incompatible heart transplantation (ABO-PE).
Data were retrospectively analysed on all ABO-incompatible heart transplants undertaken at a single centre between January 1, 2000 and June 1, 2020. Data included all routine laboratory tests, demographics and pre-operative characteristics, intraoperative details and post-operative outcomes. Primary outcome measures were volume of blood product transfusions, maximum post-transplant isohaemagglutinin titres, occurrence of rejection and graft survival. Secondary outcome measures were length of intensive care and hospital stay. Demographic and survival data were also obtained for ABO-compatible transplants during the same time period for comparison.
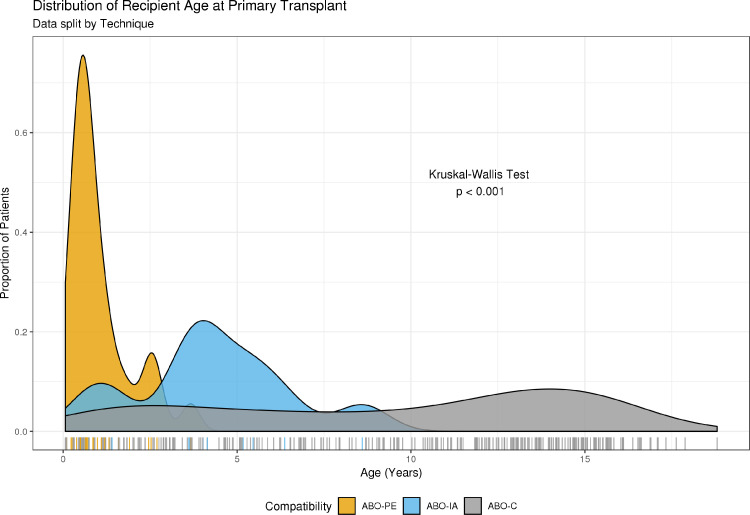
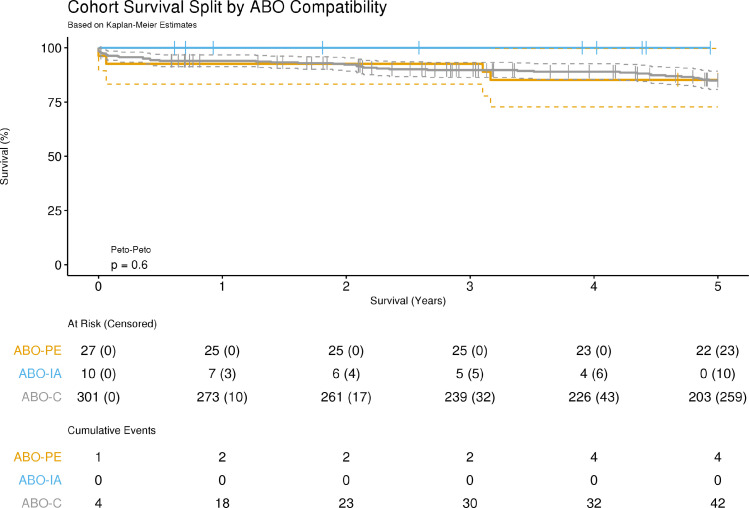
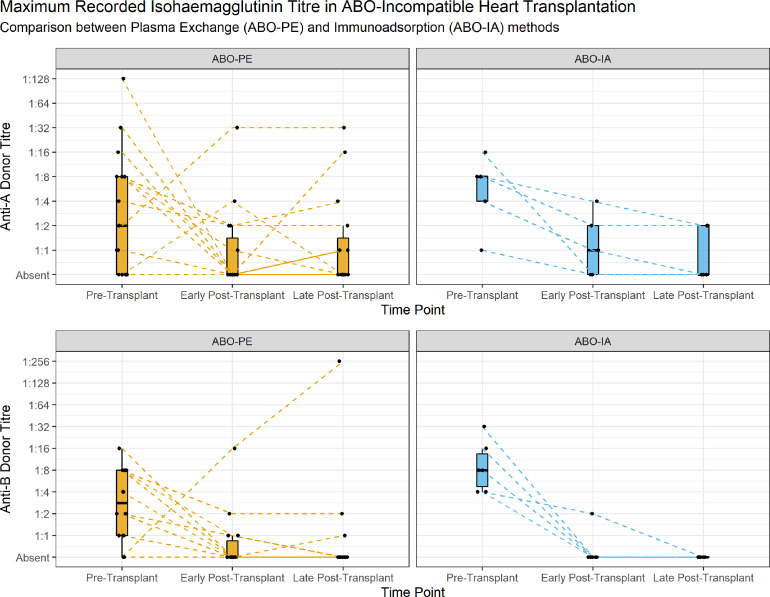
Thirty-seven patients underwent ABO-incompatible heart transplantation, with 27 (73%) using ABO-PE and 10 (27%) using ABO-IA. ABO-IA patients were significantly older than ABO-PE patients (p < 0.001) and the total volume of blood products transfused during the hospital admission was significantly lower (164 [126-212] ml/kg vs 323 [268-379] ml/kg, p < 0.001). No significant differences were noted between methods in either pre or post-transplant maximum isohaemagglutinin titres, incidence of rejection, length of intensive care or total hospital stay. Survival comparison showed no significant difference between antibody reduction methods, or indeed ABO-compatible transplants (p = 0.6).
This novel technique appears to allow a significantly older population than typical to undergo ABO-incompatible heart transplantation, as well as significantly reducing blood product utilization. Furthermore, intraoperative anti-A/B immunoadsorption does not demonstrate increased early post-transplant isohaemagglutinin accumulation or rates of rejection compared to ABO-PE. Early survival is equivalent between ABO-IA, ABO-PE and ABO-compatible heart transplantation.
术中抗 A/B 免疫吸附(ABO-IA)最近被引入用于 ABO 不相容的心脏移植。在这里,我们报告了首例接受 ABO-IA 的患者病例系列,并将结果与接受血浆置换促进 ABO 不相容心脏移植(ABO-PE)的患者进行比较。
对 2000 年 1 月 1 日至 2020 年 6 月 1 日期间在单一中心进行的所有 ABO 不相容心脏移植进行了回顾性数据分析。数据包括所有常规实验室检查、人口统计学和术前特征、术中细节和术后结果。主要观察指标是输血的血液制品量、移植后最大同种异体血凝素滴度、排斥反应的发生和移植物存活率。次要观察指标是重症监护和住院时间。同时还获得了同一时期 ABO 相容移植的人口统计学和生存数据作为比较。
37 例患者接受了 ABO 不相容心脏移植,其中 27 例(73%)采用 ABO-PE,10 例(27%)采用 ABO-IA。ABO-IA 患者明显比 ABO-PE 患者年龄大(p<0.001),住院期间输血量也明显减少(164[126-212]ml/kg 比 323[268-379]ml/kg,p<0.001)。两种方法在前或移植后最大同种异体血凝素滴度、排斥发生率、重症监护时间或总住院时间方面均无显著差异。生存比较显示,抗体减少方法之间或 ABO 相容移植之间没有显著差异(p=0.6)。
与 ABO-PE 相比,这种新的技术似乎可以让年龄比典型的患者群体接受 ABO 不相容的心脏移植,同时显著减少血液制品的使用。此外,与 ABO-PE 相比,术中抗 A/B 免疫吸附并没有增加移植后早期同种异体血凝素的积累或排斥反应的发生率。ABO-IA、ABO-PE 和 ABO 相容心脏移植的早期存活率是等效的。