Goulart Michelle R, Watt Jennifer, Siddiqui Imran, Lawlor Rita T, Imrali Ahmet, Hughes Christine, Saad Amina, ChinAleong Joanne, Hurt Chris, Cox Catrin, Salvia Roberto, Mantovani Alberto, Crnogorac-Jurcevic Tatjana, Mukherjee Somnath, Scarpa Aldo, Allavena Paola, Kocher Hemant M
Centre for Tumour Biology, Barts Cancer Institute - a CRUK Centre of Excellence, Queen Mary University of London, London, UK.
Barts and the London HPB Centre, The Royal London Hospital, Barts Health NHS Trust, London, UK.
NPJ Precis Oncol. 2021 Jun 29;5(1):61. doi: 10.1038/s41698-021-00192-1.
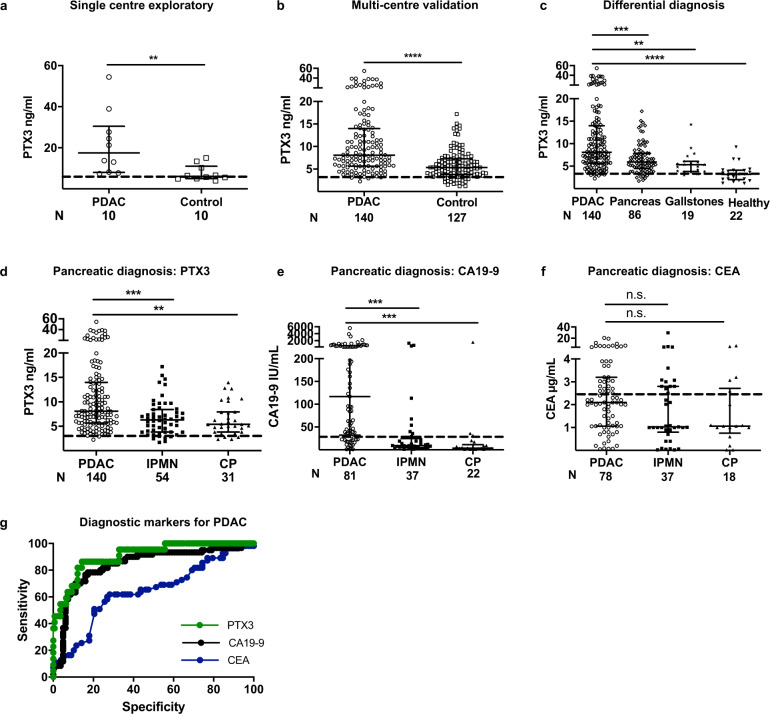
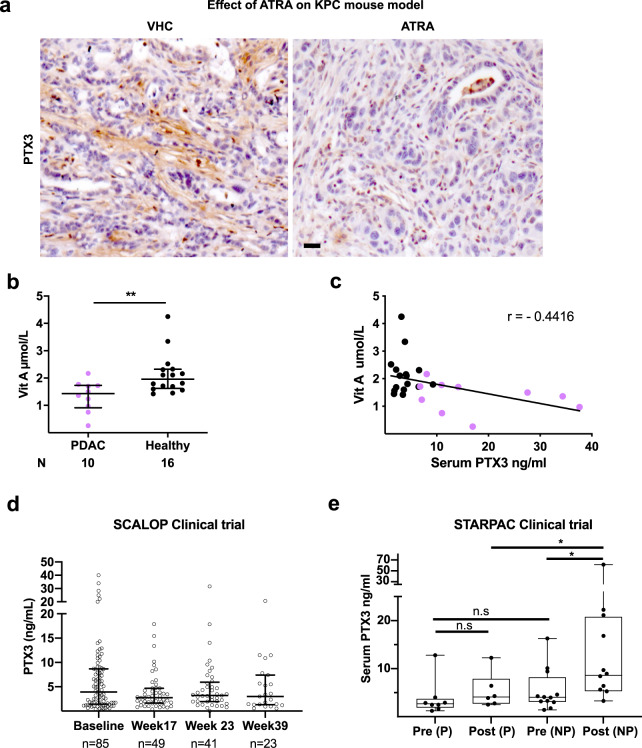
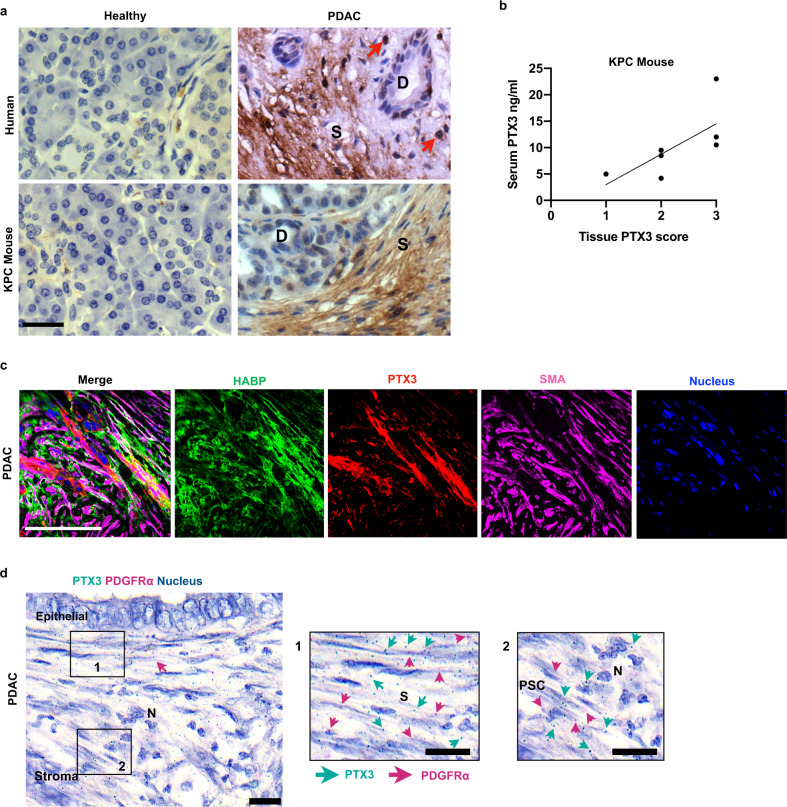
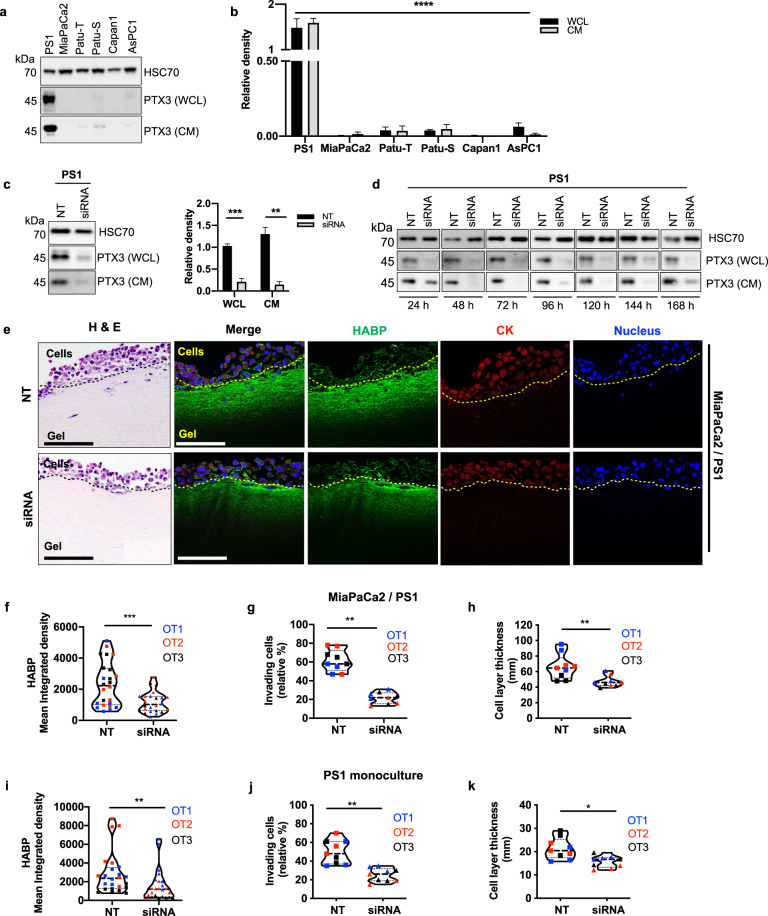
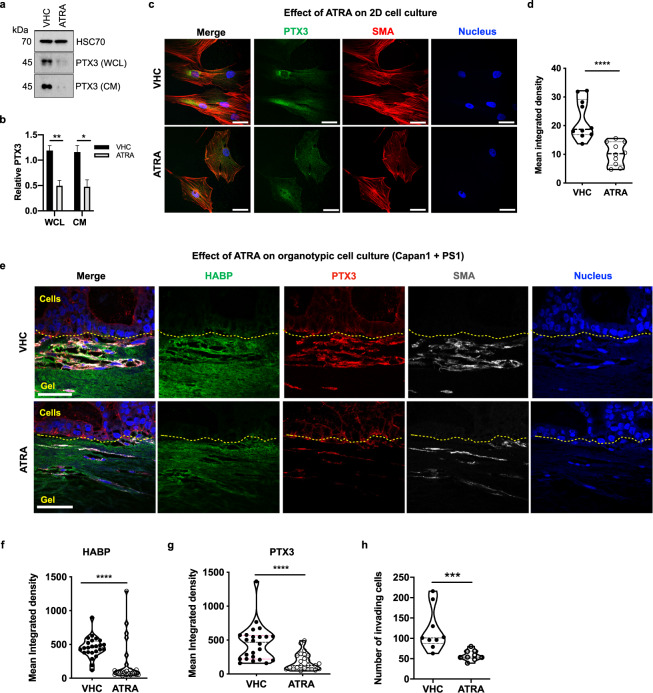
Pancreatic ductal adenocarcinoma (PDAC), characterized by dense desmoplastic stroma laid down by pancreatic stellate cells (PSC), has no reliable diagnostic biomarkers for timely detection. A multi-center cohort of PDAC patients and controls (chronic pancreatitis, intra-ductal papillary neoplasms, gallstones and otherwise healthy) donated serum in an ethically approved manner. Serum PTX3 above 4.34 ng/mL has a higher sensitivity (86%, 95% confidence interval (CI): 65-97%) and specificity (86%, 95% CI: 79-91%), positive predictive value (97%) and likelihood ratio (6.05), and is superior when compared to serum CA19-9 and CEA for detection of PDAC. In vitro and ex vivo analyses of PTX3, in human PDAC samples, PSCs, cell lines and transgenic mouse model for PDAC, suggest that PTX3 originates from stromal cells, mainly PSC. In activated PSC, PTX3 secretion could be downregulated by rendering PSC quiescent using all-trans-retinoic acid (ATRA). PTX3 organizes hyaluronan in conjunction with tumor necrosis factor-stimulated gene 6 (TSG-6) and facilitates stellate and cancer cell invasion. In SCALOP clinical trial (ISRCTN96169987) testing chemo-radiotherapy without stromal targeting, PTX3 had no prognostic or predictive role. However, in STARPAC clinical trial (NCT03307148), stromal modulation by ATRA even at first dose is accompanied with serum PTX3 response in patients who later go on to demonstrate disease control but not those in whom the disease progresses. PTX3 is a putative stromally-derived biomarker for PDAC which warrants further testing in prospective, larger, multi-center cohorts and within clinical trials targeting stroma.
胰腺导管腺癌(PDAC)的特征是由胰腺星状细胞(PSC)形成致密的促纤维增生性基质,目前尚无可靠的诊断生物标志物用于早期检测。一项多中心队列研究中,PDAC患者及对照者(慢性胰腺炎、导管内乳头状瘤、胆结石患者以及健康人)以符合伦理规范的方式捐献了血清。血清PTX3水平高于4.34 ng/mL时,其敏感性更高(86%,95%置信区间(CI):65-97%),特异性为86%(95%CI:79-91%),阳性预测值为97%,似然比为6.05,与血清CA19-9和CEA相比,在检测PDAC方面更具优势。对人PDAC样本、PSC、细胞系及PDAC转基因小鼠模型进行的PTX3体外和离体分析表明,PTX3主要来源于基质细胞,尤其是PSC。在活化的PSC中,使用全反式维甲酸(ATRA)使PSC静止可下调PTX3的分泌。PTX3与肿瘤坏死因子刺激基因6(TSG-6)共同作用组织透明质酸,促进星状细胞和癌细胞的侵袭。在不进行基质靶向的放化疗SCALOP临床试验(ISRCTN96169987)中,PTX3无预后或预测作用。然而,在STARPAC临床试验(NCT03307148)中,即使在首次给药时,ATRA对基质的调节也伴随着血清PTX3反应,后续疾病得到控制的患者出现此反应,而疾病进展的患者则未出现。PTX3是一种假定的源自基质的PDAC生物标志物,值得在前瞻性、更大规模的多中心队列研究以及针对基质的临床试验中进一步验证。