Krishna Vamshi, Govil Nishith, Tripathi Mukesh, Jain Gaurav, Goyal Tarun, Aggarwal Shantanu
Department of Anaesthesiology All India Institute of Medical Sciences, Rishikesh, India.
Department of Anaesthesiology Shri Guru Ram Rai Institute of Medical and Health Sciences, Dehradun, Uttarakhand, India.
Indian J Anaesth. 2021 May;65(Suppl 2):S80-S85. doi: 10.4103/ija.IJA_1317_20. Epub 2021 May 10.
Pain perception and pain threshold vary from one individual to another and also differ in the right and left limbs leading to an inter-cerebral pain variability bias and inter-patient pain variability bias. To date, data comparing adductor canal block (ACB) with femoral nerve block (FNB) in the same patient who underwent bilateral total knee arthroplasty (TKA) remain limited.
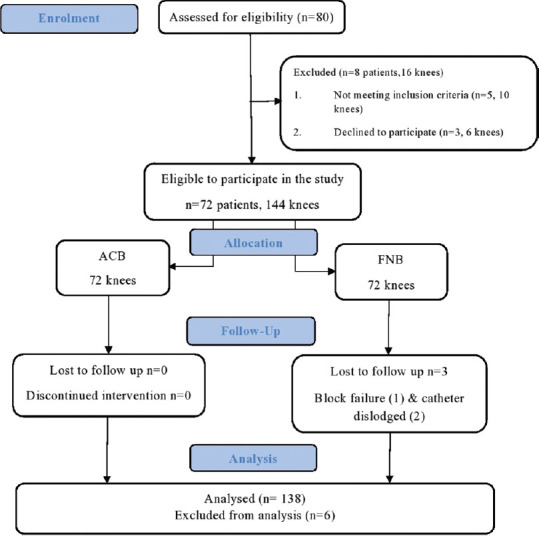
We performed a prospective, non-randomised, controlled study. Patients scheduled for bilateral TKA with central neuraxial anaesthesia received every 12-hourly intermittent boluses of 15 mL of ropivacaine 0.5% in two different peripheral nerve blocks (ACB and FNB) in either of the lower limbs postoperatively. The primary outcome was to assess postoperative VAS score, and the secondary outcomes were muscle strength of the quadriceps muscle and degree of flexion at the knee joint.
Among the 80 patients assessed for eligibility, 72 patients were enroled, and 69 were included in the final analysis. VAS scores after the two blocks during rest at 30 minutes, 6 hours, 12 hours and 48 hours post-operatively had no significant difference. VAS scores during rest at 24 hours and on doing exercise at 24 hours and 48 hours showed a significant difference. Quadriceps muscle strength and degree of flexion of knee at 24 hours and 48 hours post-operatively did show a significant difference in favour of the ACB over FNB.
ACB provides equivalent analgesia in comparison with FNB at rest and during passive exercise up to 48 hours post-operatively. ACB significantly preserved motor power of quadriceps muscles when compared with FNB with no added complications.
疼痛感知和疼痛阈值因人而异,且左右肢体也存在差异,从而导致脑间疼痛变异性偏差和患者间疼痛变异性偏差。迄今为止,在接受双侧全膝关节置换术(TKA)的同一患者中比较内收肌管阻滞(ACB)与股神经阻滞(FNB)的资料仍然有限。
我们进行了一项前瞻性、非随机对照研究。计划接受双侧TKA并采用椎管内麻醉的患者,术后在双下肢的两种不同外周神经阻滞(ACB和FNB)中,每12小时接受一次15 mL 0.5%罗哌卡因的间歇性推注。主要结局是评估术后视觉模拟评分(VAS),次要结局是股四头肌肌力和膝关节屈曲程度。
在80例评估 eligibility的患者中,72例入组,69例纳入最终分析。术后30分钟、6小时、12小时和48小时静息时两种阻滞的VAS评分无显著差异。术后24小时静息时以及24小时和48小时运动时的VAS评分有显著差异。术后24小时和48小时股四头肌肌力和膝关节屈曲程度在ACB组优于FNB组,差异有统计学意义。
ACB与FNB相比,在术后48小时内静息和被动运动时提供同等的镇痛效果。与FNB相比,ACB显著保留了股四头肌的运动能力,且无额外并发症。