National Centre for Infectious Diseases, Singapore.
National University of Singapore, Singapore.
Medicine (Baltimore). 2021 Jul 2;100(26):e26507. doi: 10.1097/MD.0000000000026507.
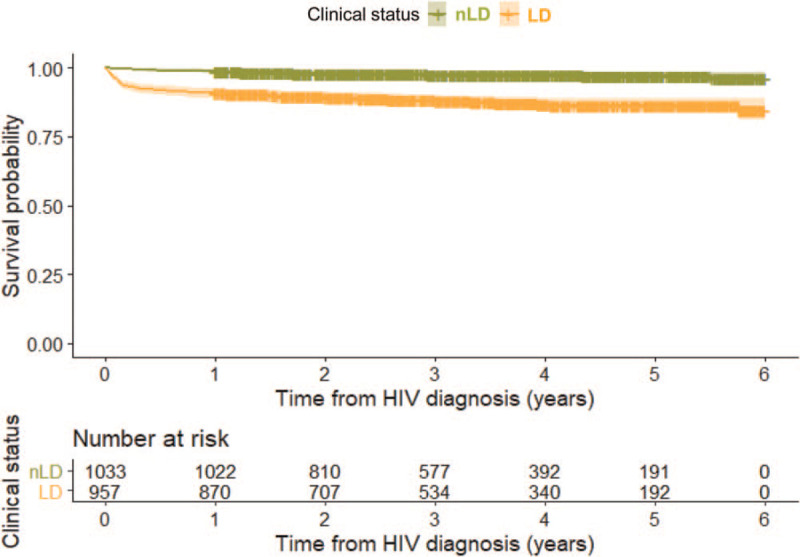
We investigated the temporal trends of short-term mortality (death within 1 year of diagnosis) and cause-specific deaths in human immunodeficiency virus (HIV)-infected persons by stage of HIV infection at diagnosis. We also assessed the impact of late diagnosis (LD) on short-term mortality.Epidemiological records of HIV-infected Singapore residents from the National HIV Registry were linked to death records from the Registry of Births and Deaths for observational analyses. Newly-diagnosed HIV cases with available cluster of differentiation 4 count at time of diagnosis in a 5-year period from 2012 to 2016 were included in the study. Hazard ratios (HRs) and 95% confidence interval (CI) of LD for all deaths excluding suicides and self-inflicted or accidental injuries, and HIV/ acquired immunodeficiency syndrome (AIDS)-related deaths occurring within 1 year post-diagnosis were calculated using Cox proportional hazards regression models with adjustment for age at HIV/AIDS diagnosis. Population attributable risk proportions (PARPs) were then calculated using the adjusted HRs.Of the 1990 newly-diagnosed HIV cases included in the study, 7.2% had died by end of 2017, giving an overall mortality rate of 2.16 per 100 person-years (PY) (95% CI 1.82-2.54). The mortality rate was 3.81 per 100 PY (95% CI 3.15-4.56) in HIV cases with LD, compared with 0.71 (95% CI 0.46-1.05) in non-LD (nLD) cases. Short-term mortality was significantly higher in LD (9.1%) than nLD cases (1.1%). Of the 143 deaths reported between 2012 and 2017, 58.0% were HIV/AIDS-related (nLD 28.0% vs LD 64.4%). HIV/AIDS-related causes represented 70.4% of all deaths which occurred during the first year of diagnosis (nLD 36.4% vs LD 74.7%). The PARP of short-term mortality due to LD was 77.8% for all deaths by natural causes, and 87.8% for HIV/AIDS-related deaths.The mortality rate of HIV-infected persons with LD was higher than nLD, especially within 1 year of diagnosis, and HIV/AIDS-related causes constituted majority of these deaths. To reduce short-term mortality, persons at high risk of late-stage HIV infection should be targeted in outreach efforts to promote health screening and remove barriers to HIV testing and treatment.
我们通过诊断时 HIV 感染阶段调查了 HIV 感染者短期死亡率(诊断后 1 年内死亡)和特定病因死亡率的时间趋势。我们还评估了晚期诊断(LD)对短期死亡率的影响。从 2012 年至 2016 年的 5 年期间,对来自国家 HIV 登记处的 HIV 感染新加坡居民的流行病学记录与死亡登记处的死亡记录进行了关联,以进行观察性分析。本研究纳入了新诊断 HIV 病例,在诊断时具有可用的 CD4 计数,并且在 2012 年至 2016 年的 5 年期间内有诊断记录。使用 Cox 比例风险回归模型计算了所有死亡(不包括自杀、自残或意外损伤)和诊断后 1 年内发生的 HIV/AIDS 相关死亡的 LD 风险比(HR)和 95%置信区间(CI),调整了 HIV/AIDS 诊断时的年龄。然后,使用调整后的 HR 计算了人群归因风险比例(PARP)。在纳入研究的 1990 例新诊断 HIV 病例中,截至 2017 年底,7.2%的病例死亡,总死亡率为每 100 人年(PY)2.16 例(95%CI 1.82-2.54)。LD 组的死亡率为每 100 PY 3.81(95%CI 3.15-4.56),而非 LD(nLD)组为 0.71(95%CI 0.46-1.05)。LD 组的短期死亡率(9.1%)明显高于 nLD 组(1.1%)。在 2012 年至 2017 年期间报告的 143 例死亡中,58.0%与 HIV/AIDS 相关(nLD 28.0%与 LD 64.4%)。在诊断后第一年发生的所有死亡中,HIV/AIDS 相关病因占 70.4%(nLD 36.4%与 LD 74.7%)。LD 导致的所有自然原因短期死亡率的 PARP 为 77.8%,HIV/AIDS 相关死亡的 PARP 为 87.8%。LD 组 HIV 感染者的死亡率高于 nLD 组,尤其是在诊断后 1 年内,HIV/AIDS 相关病因构成了这些死亡的主要原因。为了降低短期死亡率,应针对 HIV 感染晚期风险较高的人群开展外展工作,以促进健康筛查并消除 HIV 检测和治疗的障碍。