Institute for Global Health, University College London, London, UK.
National Institute for Health Research (NIHR) Health Protection Research Unit (HPRU) in Blood Borne and Sexually Transmitted Infections, University College London, London, UK.
HIV Med. 2022 Dec;23(11):1163-1172. doi: 10.1111/hiv.13436. Epub 2022 Nov 20.
Despite improvements in survival of people with HIV admitted to the intensive care unit (ICU), late diagnosis continues to contribute to in-ICU mortality. We quantify the population attributable fraction (PAF) of in-ICU mortality for recent late diagnosis among people with HIV admitted to a London ICU.
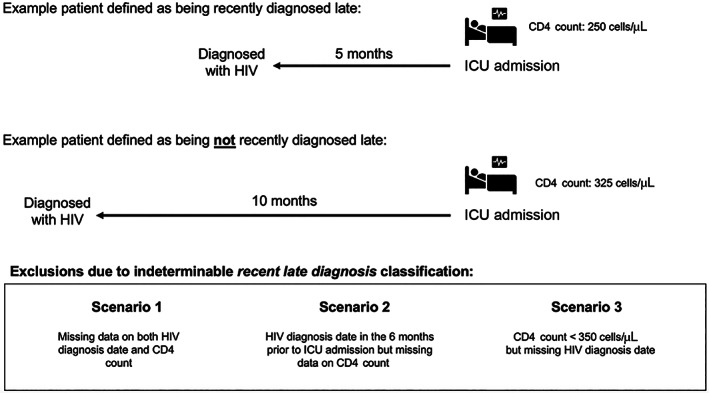
Index ICU admissions among people with HIV were considered from 2000 to 2019. Recent late diagnosis was a CD4 T-cell count < 350 cells/μL and/or AIDS-defining illness at/within 6 months prior to ICU admission. Univariate comparisons were conducted using Wilcoxon rank-sum/Cochran-Armitage/χ /Fisher's exact tests. We used Poisson regression (robust standard errors) to estimate unadjusted/adjusted (age, sex, calendar year of ICU admission) risk ratios (RRs) and regression standardization to estimate the PAF.
In all, 207 index admissions were included [median (interquartile range) age: 46 (38-53) years; 72% male]; 58 (28%) had a recent late diagnosis, all of whom had a CD4 count < 350 cells/μL, and 95% had advanced HIV (CD4 count < 200 cells/μL and/or AIDS at admission) as compared with 57% of those who did not have a recent late diagnosis (p < 0.001). In-ICU mortality was 27% (55/207); 38% versus 22% in those who did and did not have a recent late diagnosis, respectively (p = 0.02). Recent late diagnosis was independently associated with increased in-ICU mortality risk (adjusted RR = 1.75) (95% confidence interval: 1.05-2.91), with 17.08% (16.04-18.12%) of deaths being attributable to this.
There is a need for improved public health efforts focused on HIV testing and reporting of late diagnosis to better understand potentially missed opportunities for earlier HIV diagnosis in healthcare services.
尽管接受重症监护病房(ICU)治疗的艾滋病毒感染者的生存率有所提高,但晚期诊断仍导致 ICU 死亡率升高。我们量化了伦敦 ICU 收治的艾滋病毒感染者中近期晚期诊断导致 ICU 死亡的人群归因分数(PAF)。
本研究纳入了 2000 年至 2019 年期间 ICU 入院的艾滋病毒感染者。近期晚期诊断定义为 CD4 细胞计数 < 350 个/μL 和/或 AIDS 定义性疾病在 ICU 入院前 6 个月内发生。采用 Wilcoxon 秩和检验/Cochran-Armitage 检验/卡方检验进行单因素比较。采用泊松回归(稳健标准差)估计未调整/调整(年龄、性别、ICU 入院年份)风险比(RR),采用回归标准化估计 PAF。
共纳入 207 例 ICU 入院,中位(四分位间距)年龄为 46(38-53)岁,72%为男性;58 例(28%)有近期晚期诊断,所有患者 CD4 细胞计数 < 350 个/μL,95%有晚期 HIV(CD4 细胞计数 < 200 个/μL 和/或入院时 AIDS),而无近期晚期诊断的患者中这一比例为 57%(p < 0.001)。ICU 死亡率为 27%(55/207),近期晚期诊断者死亡率为 38%,而非近期晚期诊断者死亡率为 22%(p = 0.02)。近期晚期诊断与 ICU 死亡率增加独立相关(调整 RR = 1.75)(95%置信区间:1.05-2.91),17.08%(16.04-18.12%)的死亡归因于该诊断。
需要加强公共卫生努力,重点关注 HIV 检测和报告晚期诊断,以更好地了解在医疗保健服务中可能错失的早期 HIV 诊断机会。