Thannhauser Jos, Nas Joris, Vart Priya, Smeets Joep L R M, de Boer Menko-Jan, van Royen Niels, Bonnes Judith L, Brouwer Marc A
Department of Cardiology, Radboud University Medical Center, Geert Grooteplein Zuid 10, 6525 GA Nijmegen, The Netherlands.
Department of Health Evidence, Radboud University Medical Center, Geert Grooteplein Zuid 10, 6525 GA Nijmegen, The Netherlands.
Resusc Plus. 2021 Apr 2;6:100114. doi: 10.1016/j.resplu.2021.100114. eCollection 2021 Jun.
In cardiac arrest, ventricular fibrillation (VF) waveform analysis has identified the amplitude spectrum area (AMSA) as a key predictor of defibrillation success and favorable neurologic survival. New resuscitation protocols are under investigation, where prompt defibrillation is restricted to cases with a high AMSA. Appreciating the variability of in-field pad placement, we aimed to assess the impact of recording direction on AMSA-values, and the inherent defibrillation advice.
Prospective VF-waveform study on 12-lead surface electrocardiograms (ECGs) obtained during defibrillation testing in ICD-recipients (2010-2017). AMSA-values (mVHz) of simultaneous VF-recordings were calculated and compared between all limb leads, with lead II as reference (proxy for in-field pad position). AMSA-differences between leads I and II were quantified using Bland-Altman analysis. Moreover, we investigated differences between these adjacent leads regarding classification into high (≥15.5), intermediate (6.5-15.5) or low (≤6.5) AMSA-values.
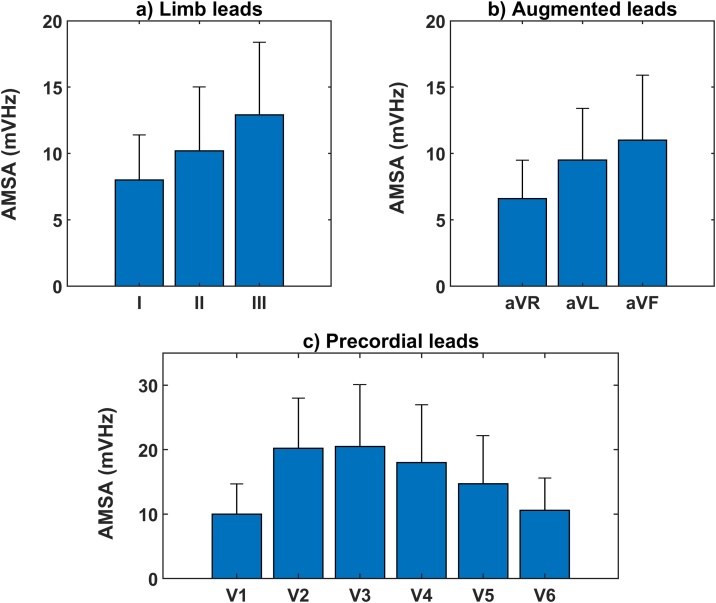
In this cohort (n = 243), AMSA-values in lead II (10.2 ± 4.8) differed significantly from the other limb leads (I: 8.0 ± 3.4; III: 12.9 ± 5.6, both p < 0.001). The AMSA-value in lead I was, on average, 2.24 ± 4.3 lower than in lead II. Of the subjects with high AMSA-values in lead II, only 15% were classified as high if based on assessments of lead I. For intermediate and low AMSA-values, concordances were 66% and 72% respectively.
ECG-recording direction markedly affects the result of VF-waveform analysis, with 20-30% lower AMSA-values in lead I than in lead II. Our data suggest that electrode positioning may significantly impact shock guidance by 'smart defibrillators', especially affecting the advice for prompt defibrillation.
在心脏骤停中,室颤(VF)波形分析已确定振幅频谱面积(AMSA)是除颤成功和良好神经功能存活的关键预测指标。新的复苏方案正在研究中,其中快速除颤仅限于AMSA值高的病例。鉴于现场电极片放置的变异性,我们旨在评估记录方向对AMSA值的影响以及固有的除颤建议。
对2010年至2017年期间在植入式心律转复除颤器(ICD)接受者的除颤测试中获得的12导联体表心电图(ECG)进行前瞻性VF波形研究。计算并比较所有肢体导联同步VF记录的AMSA值(mVHz),以II导联作为参考(代表现场电极片位置)。使用Bland-Altman分析量化I导联和II导联之间的AMSA差异。此外,我们研究了这些相邻导联在分类为高(≥15.5)、中(6.5-15.5)或低(≤6.5)AMSA值方面的差异。
在该队列(n = 243)中,II导联的AMSA值(10.2±4.8)与其他肢体导联(I导联:8.0±3.4;III导联:12.9±5.6,均p < 0.001)有显著差异。I导联的AMSA值平均比II导联低2.24±4.3。在II导联AMSA值高的受试者中,如果基于I导联评估,只有15%被分类为高。对于中、低AMSA值,一致性分别为66%和72%。
心电图记录方向显著影响VF波形分析结果,I导联的AMSA值比II导联低20%-30%。我们的数据表明,电极定位可能会显著影响“智能除颤器”的电击指导,特别是影响快速除颤的建议。