Institute for Trauma Recovery, University of North Carolina, Chapel Hill, NC, USA.
Department of Anesthesiology, University of North Carolina, Chapel Hill, NC, USA.
Transl Psychiatry. 2021 Jun 29;11(1):359. doi: 10.1038/s41398-021-01486-5.
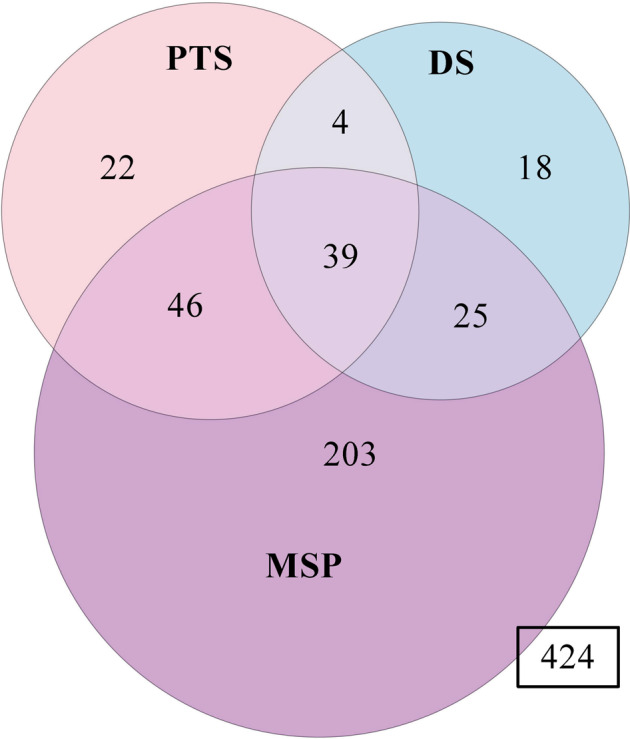
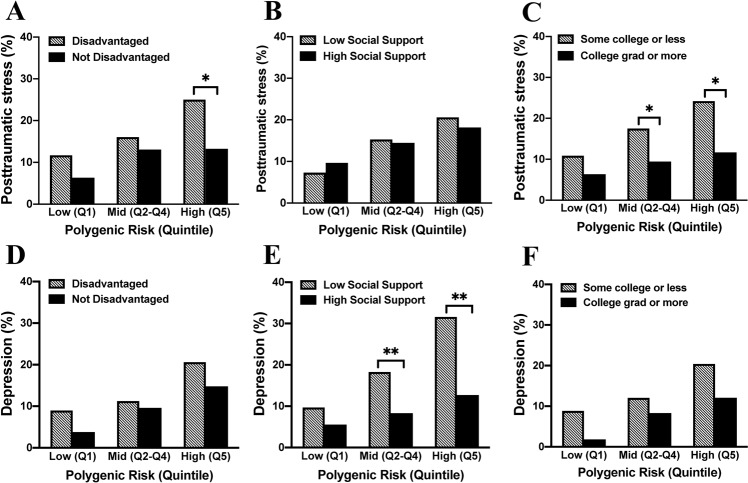
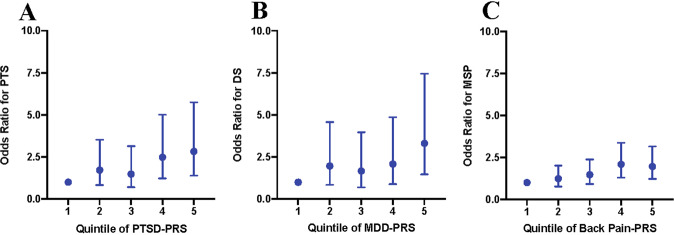
Posttraumatic stress (PTS), depressive symptoms (DS), and musculoskeletal pain (MSP) are common sequelae of trauma exposure. Although these adverse posttraumatic neuropsychiatric sequelae (APNS) are often studied separately, clinical comorbidity is high. In a cohort of European American motor vehicle collision (MVC) trauma survivors (n = 781), substantial PTS (≥33, IES-R), DS (≥26, CES-D), and MSP (≥4, 0-10 NRS) were identified via a 6-month survey. Genetic risk was estimated using polygenic risk scores (PRSs) calculated from the largest available GWAS datasets of PTSD, MDD, and back pain. We then assessed comorbidity and genetic risk influence for developing chronic PTS, DS, and MSP after MVC. Secondary analyses explored whether common social determinants of health ameliorate genetic vulnerability. We found that 6 months after MVC, nearly half 357/781 (46%) of the participants had substantial PTS, DS, and/or MSP, and overlap was common (PTS + MSP (23%), DS + MSP (18%), PTS + DS (12%)). Genetic risk predicted post-MVC outcomes. PTSD-PRSs predicted PTS and DS (R = 2.21% and 2.77%, p < 0.01), MDD-PRSs predicted DS and MSP (R = 1.89%, p < 0.01) and 0.79%, p < 0.05), and back pain-PRS predicted MSP (R = 1.49%, p < 0.01). Individuals in the highest quintile of PTSD-PRSs had 2.8 and 3.5 times the odds of developing PTS and DS vs. the lowest quintile (95% CI = 1.39-5.75 and 1.58-7.76). Among these high-risk individuals, those living in non-disadvantaged neighborhoods and with college education had 47% (p = 0.048) and 52% (p = 0.04) less risk of developing PTS, and those with high social support had 60% (p = 0.008) less risk of developing DS. Overall, genetic factors influence the risk of APNS after MVC, genetic risk of distinct APNS are overlapping, and specific social determinants greatly augment genetic risk of APNS development after MVC.
创伤后应激(PTS)、抑郁症状(DS)和肌肉骨骼疼痛(MSP)是创伤暴露的常见后遗症。尽管这些不良的创伤后神经精神后遗症(APNS)通常是分开研究的,但临床上的合并症很高。在一项欧洲裔美国机动车碰撞(MVC)创伤幸存者队列研究中(n=781),通过 6 个月的调查确定了大量 PTS(≥33,IES-R)、DS(≥26,CES-D)和 MSP(≥4,0-10 NRS)。使用从 PTSD、MDD 和背痛最大可用 GWAS 数据集计算的多基因风险评分(PRSs)来估计遗传风险。然后,我们评估了 MVC 后慢性 PTS、DS 和 MSP 发病的合并症和遗传风险影响。次要分析探讨了常见的健康社会决定因素是否能减轻遗传易感性。我们发现,在 MVC 后 6 个月,近一半的 357/781(46%)参与者有大量 PTS、DS 和/或 MSP,并且重叠很常见(PTS+MSP(23%),DS+MSP(18%),PTS+DS(12%))。遗传风险预测了 MVC 后的结果。PTSD-PRS 预测 PTS 和 DS(R=2.21%和 2.77%,p<0.01),MDD-PRS 预测 DS 和 MSP(R=1.89%,p<0.01)和 0.79%,p<0.05)和背痛-PRS 预测 MSP(R=1.49%,p<0.01)。PTSD-PRS 最高五分位数的个体患 PTS 和 DS 的可能性是最低五分位数的个体的 2.8 和 3.5 倍(95%CI=1.39-5.75 和 1.58-7.76)。在这些高风险个体中,居住在非贫困社区和受过大学教育的个体患 PTS 的风险分别降低了 47%(p=0.048)和 52%(p=0.04),而社会支持度高的个体患 DS 的风险降低了 60%(p=0.008)。总的来说,遗传因素影响 MVC 后 APNS 的风险,不同 APNS 的遗传风险是重叠的,特定的社会决定因素大大增加了 MVC 后 APNS 发展的遗传风险。