Department of Biology, Faculty of Sciences, Kyushu University, Fukuoka, Japan.
interdisciplinary Biology Laboratory (iBLab), Division of Biological Science, Graduate School of Science, Nagoya University, Nagoya, Japan.
PLoS Med. 2021 Jul 6;18(7):e1003660. doi: 10.1371/journal.pmed.1003660. eCollection 2021 Jul.
Development of an effective antiviral drug for Coronavirus Disease 2019 (COVID-19) is a global health priority. Although several candidate drugs have been identified through in vitro and in vivo models, consistent and compelling evidence from clinical studies is limited. The lack of evidence from clinical trials may stem in part from the imperfect design of the trials. We investigated how clinical trials for antivirals need to be designed, especially focusing on the sample size in randomized controlled trials.
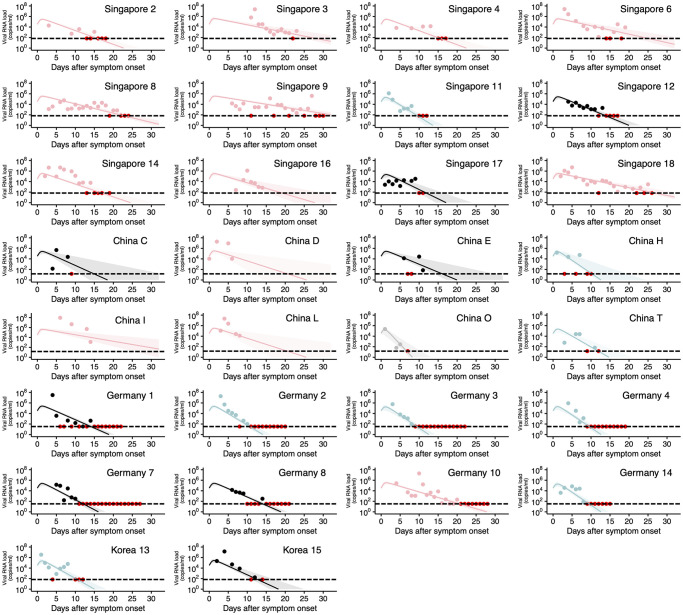
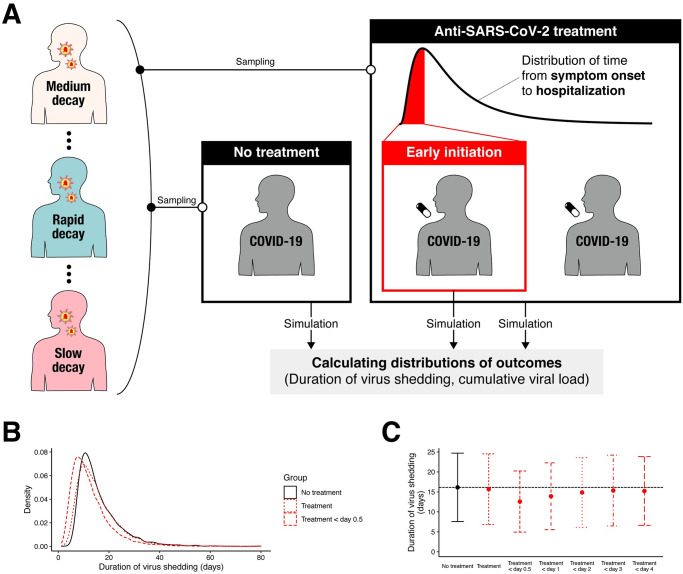
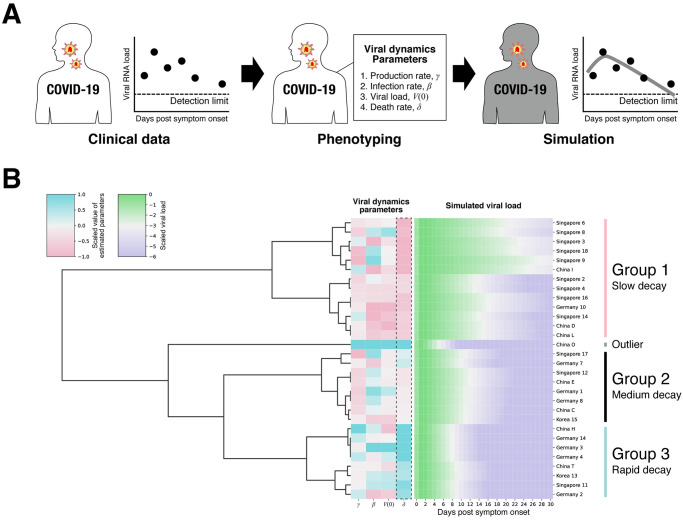
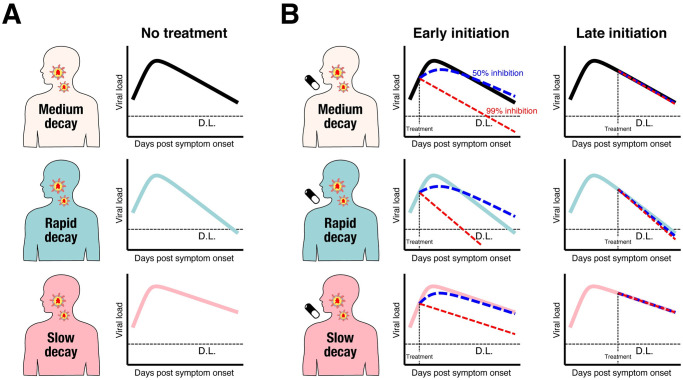
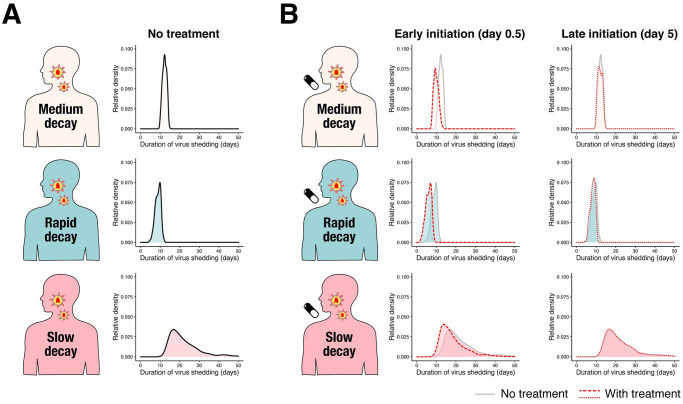
A modeling study was conducted to help understand the reasons behind inconsistent clinical trial findings and to design better clinical trials. We first analyzed longitudinal viral load data for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) without antiviral treatment by use of a within-host virus dynamics model. The fitted viral load was categorized into 3 different groups by a clustering approach. Comparison of the estimated parameters showed that the 3 distinct groups were characterized by different virus decay rates (p-value < 0.001). The mean decay rates were 1.17 d-1 (95% CI: 1.06 to 1.27 d-1), 0.777 d-1 (0.716 to 0.838 d-1), and 0.450 d-1 (0.378 to 0.522 d-1) for the 3 groups, respectively. Such heterogeneity in virus dynamics could be a confounding variable if it is associated with treatment allocation in compassionate use programs (i.e., observational studies). Subsequently, we mimicked randomized controlled trials of antivirals by simulation. An antiviral effect causing a 95% to 99% reduction in viral replication was added to the model. To be realistic, we assumed that randomization and treatment are initiated with some time lag after symptom onset. Using the duration of virus shedding as an outcome, the sample size to detect a statistically significant mean difference between the treatment and placebo groups (1:1 allocation) was 13,603 and 11,670 (when the antiviral effect was 95% and 99%, respectively) per group if all patients are enrolled regardless of timing of randomization. The sample size was reduced to 584 and 458 (when the antiviral effect was 95% and 99%, respectively) if only patients who are treated within 1 day of symptom onset are enrolled. We confirmed the sample size was similarly reduced when using cumulative viral load in log scale as an outcome. We used a conventional virus dynamics model, which may not fully reflect the detailed mechanisms of viral dynamics of SARS-CoV-2. The model needs to be calibrated in terms of both parameter settings and model structure, which would yield more reliable sample size calculation.
In this study, we found that estimated association in observational studies can be biased due to large heterogeneity in viral dynamics among infected individuals, and statistically significant effect in randomized controlled trials may be difficult to be detected due to small sample size. The sample size can be dramatically reduced by recruiting patients immediately after developing symptoms. We believe this is the first study investigated the study design of clinical trials for antiviral treatment using the viral dynamics model.
开发针对 2019 年冠状病毒病(COVID-19)的有效抗病毒药物是全球卫生的当务之急。尽管已经通过体外和体内模型确定了几种候选药物,但来自临床研究的一致且令人信服的证据有限。临床试验证据的缺乏可能部分源于试验设计的不完善。我们研究了抗病毒药物的临床试验应如何设计,特别是重点关注随机对照试验的样本量。
进行了一项建模研究,以帮助了解临床试验结果不一致的原因,并设计更好的临床试验。我们首先使用基于宿主的病毒动力学模型分析了未经抗病毒治疗的严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)的纵向病毒载量数据。使用聚类方法将拟合的病毒载量分为 3 个不同的组。比较估计参数表明,这 3 个不同的组具有不同的病毒衰减率(p 值<0.001)。平均衰减率分别为 1.17 d-1(95%CI:1.06 至 1.27 d-1)、0.777 d-1(0.716 至 0.838 d-1)和 0.450 d-1(0.378 至 0.522 d-1),分别为 3 个组。如果这种病毒动力学的异质性与同情使用计划(即观察性研究)中的治疗分配相关,则可能是混杂变量。随后,我们通过模拟模拟了抗病毒药物的随机对照试验。向模型中添加了导致病毒复制减少 95%至 99%的抗病毒作用。为了现实起见,我们假设随机化和治疗在症状出现后经过一定的时间延迟开始。使用病毒脱落的持续时间作为结果,如果所有患者都被纳入(无论随机化时间如何),则每组检测治疗组和安慰剂组之间统计学上有显著差异的样本量为 13603 和 11670(当抗病毒作用分别为 95%和 99%时)。如果仅纳入症状出现后 1 天内接受治疗的患者,则样本量减少至 584 和 458(当抗病毒作用分别为 95%和 99%时)。我们确认当使用对数标度的累积病毒载量作为结果时,样本量也会相应减少。我们使用了常规的病毒动力学模型,该模型可能无法充分反映 SARS-CoV-2 病毒动力学的详细机制。模型需要在参数设置和模型结构方面进行校准,这将产生更可靠的样本量计算。
在这项研究中,我们发现观察性研究中估计的关联可能因受感染个体中病毒动力学的较大异质性而存在偏差,并且由于样本量小,随机对照试验中的统计学显著效果可能难以检测到。通过在出现症状后立即招募患者,可以大大减少样本量。我们相信这是第一项使用病毒动力学模型研究抗病毒治疗临床试验设计的研究。