Department of Emergency Medicine, Beijing Chaoyang Hospital Jingxi Branch, Capital Medical University, No.5 Jingyuan Road, Shijingshan, Beijing, 100043, China.
BMC Emerg Med. 2021 Jul 7;21(1):81. doi: 10.1186/s12873-021-00477-5.
Evidence suggests that C-reactive protein (CRP), procalcitonin (PCT), and immune cells can predict sepsis severity in adult patients. However, the specific values of these indicators are not consistent in predicting prognosis.
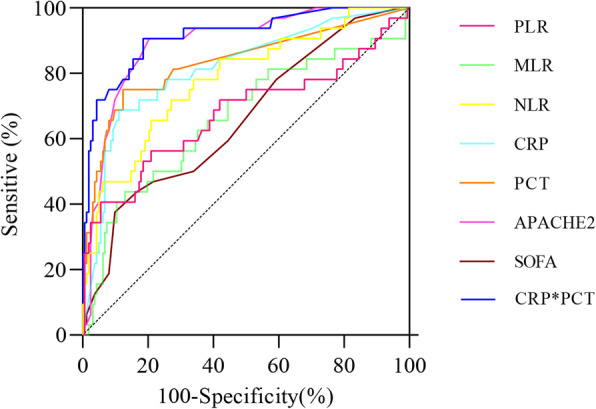
A retrospective study analyzed the medical records of 194 patients based on the concept of sepsis in 2016 (Sepsis 3.0) from January 2017 to December 2019. A comparative analysis of inflammatory factors associated with patients in the sepsis survival and the non-survival group was performed. The concentrations of CRP and PCT, neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), and platelet-to-lymphocyte ratio (PLR) were measured. ROC curve was used to assess the diagnosis and analysis of the selected indices of sepsis. According to each index's cut-off value of the ROC curve, the patients were divided into two groups, and the prognosis was calculated.
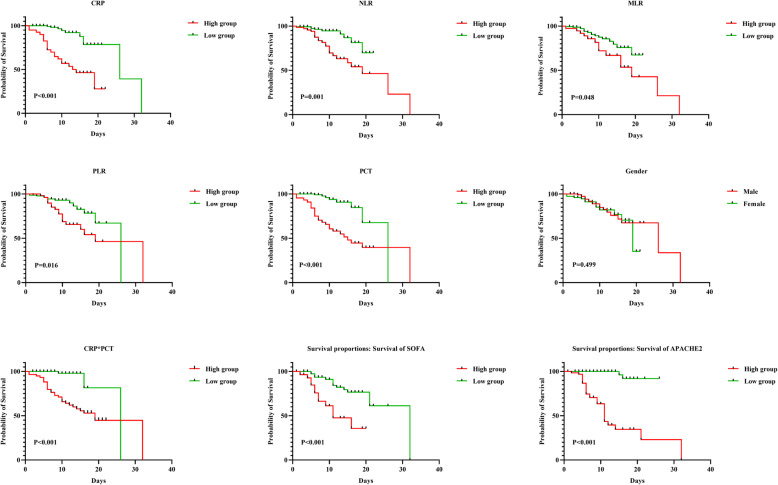
Among the 194 patients, 32 died (16.49%), the median age of the patients was 79 (66.0, 83.3) years, and 118 were male (60.8%). Analysis of related inflammatory indicators showed that CRP, NLR, MLR, PLR, and CRPPCT in the non-survival group were statistically higher than those in the survival group (all p values were < 0.05). Regression analysis showed that PCT, CRP, NLR, PLR, and CRPPCT were all independent prognostic factors for patients. The ROC curve results showed that CRPPCT had the best diagnostic value (AUC = 0.915). The cut-off values of PCT, CRP, NLR, PLR, MLR, and CRPPCT were 0.25 ng/mL, 85.00 mg/L, 8.66, 275.51, 0.74%, and 5.85 (mg/L), respectively. Kaplan-Meier survival estimate showed that patient prognosis between the CRP, PCT, NLR, PLR, and CRP*PCT was statistically different (all values P < 0.05, respectively). However, there was no statistically significant difference in gender and MLR (all values P > 0.05, respectively), grouping based on diagnostic cut-off values.
In this study, inflammation-related markers PCT, CRP, NLR, MLR, PLR, and CRP*PCT can be used as independent risk factors affecting the prognosis of patients with sepsis. Furthermore, except for MRL, these indicators have cut-off values for predicting patient death.
有证据表明,C 反应蛋白(CRP)、降钙素原(PCT)和免疫细胞可预测成人脓毒症的严重程度。然而,这些指标在预测预后方面的具体价值并不一致。
回顾性研究分析了 2017 年 1 月至 2019 年 12 月间根据 2016 年脓毒症概念(脓毒症 3.0)的 194 例患者的病历。对存活组和非存活组患者的炎症因子进行了对比分析。测量了 CRP 和 PCT、中性粒细胞与淋巴细胞比值(NLR)、单核细胞与淋巴细胞比值(MLR)和血小板与淋巴细胞比值(PLR)的浓度。使用 ROC 曲线评估了脓毒症相关指标的诊断和分析。根据 ROC 曲线各指标的截断值,将患者分为两组,计算预后。
194 例患者中,32 例死亡(16.49%),患者中位年龄为 79(66.0,83.3)岁,118 例为男性(60.8%)。对相关炎症指标进行分析显示,非存活组的 CRP、NLR、MLR、PLR 和 CRPPCT 均明显高于存活组(均 P 值<0.05)。回归分析显示,PCT、CRP、NLR、PLR 和 CRPPCT 均为患者的独立预后因素。ROC 曲线结果表明,CRPPCT 具有最佳的诊断价值(AUC=0.915)。PCT、CRP、NLR、PLR、MLR 和 CRPPCT 的截断值分别为 0.25ng/mL、85.00mg/L、8.66、275.51、0.74%和 5.85(mg/L)。Kaplan-Meier 生存估计表明,CRP、PCT、NLR、PLR 和 CRP*PCT 之间患者的预后存在统计学差异(均 P 值<0.05)。然而,性别和 MLR 分组在诊断截断值方面没有统计学差异(均 P 值>0.05)。
在本研究中,炎症相关标志物 PCT、CRP、NLR、MLR、PLR 和 CRP*PCT 可作为影响脓毒症患者预后的独立危险因素。此外,除 MRL 外,这些指标均有预测患者死亡的截断值。