Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, Texas.
Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston, Texas.
Cancer. 2021 Oct 15;127(20):3772-3781. doi: 10.1002/cncr.33689. Epub 2021 Jul 13.
TP53 mutation (TP53 ) confers an adverse prognosis in acute myeloid leukemia (AML). Venetoclax with hypomethylating agents is a current standard for older patients; however, recent reports suggest that TP53 confers resistance to venetoclax. The authors investigated the outcomes of patients with TP53 AML who were treated with a 10-day decitabine and venetoclax (DEC10-VEN) (ClinicalTrials.gov identifier NCT03404193).
Patients with newly diagnosed AML received decitabine 20 mg/m for 10 days every 4 to 6 weeks for induction, followed by decitabine for 5 days after response. The venetoclax dose was 400 mg daily. TP53 was identified in bone marrow samples using next-generation sequencing, with sensitivity of 5%. Outcomes were analyzed according to European LeukemiaNet 2017 guidelines.
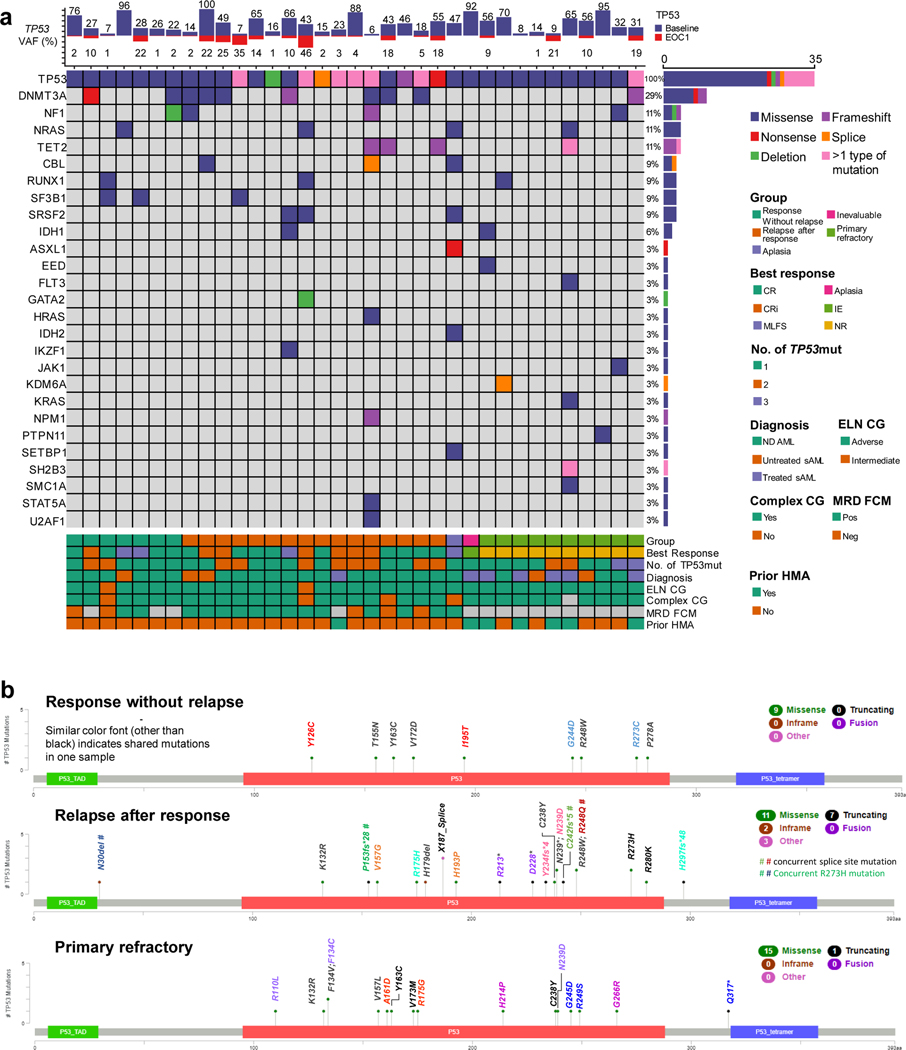
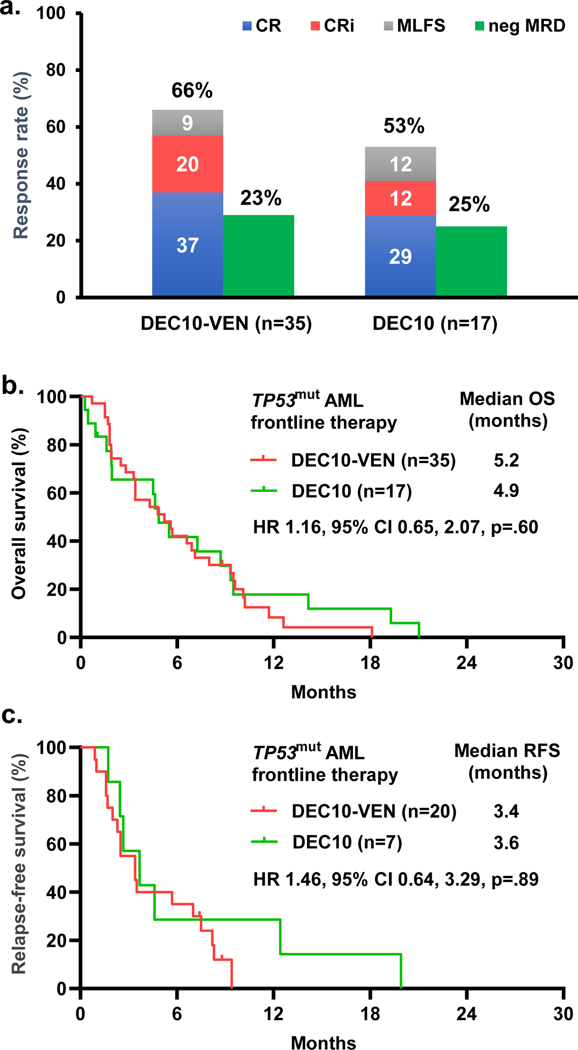
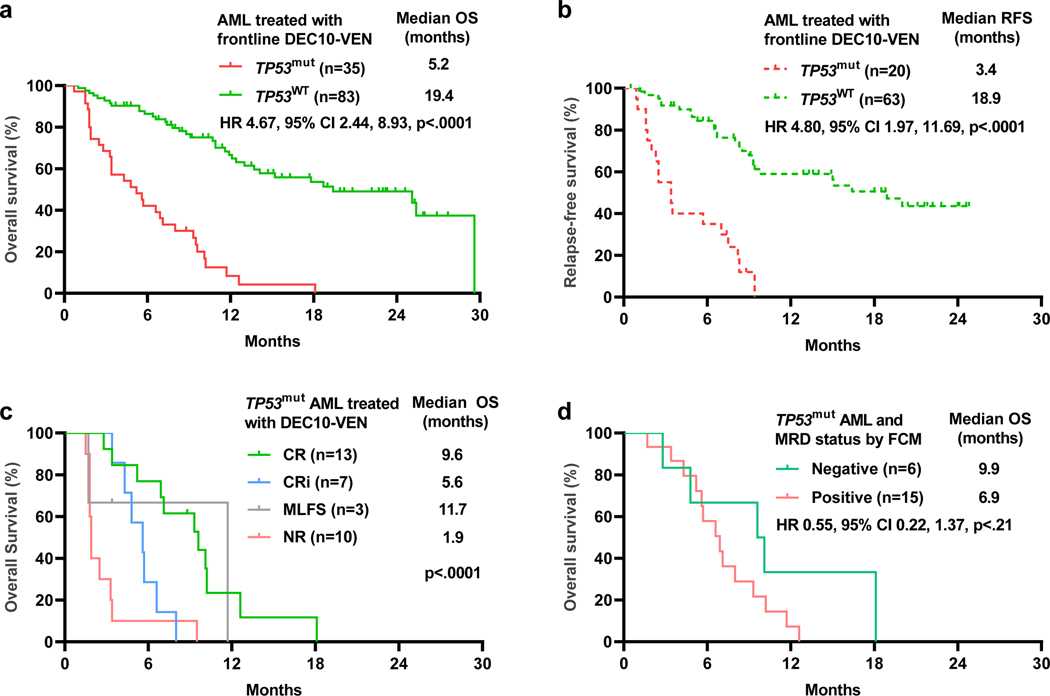
Among 118 patients (median age, 72 years; age range, 49-89 years), 63 (53%) had secondary AML, 39 (33%) had AML with complex karyotype, and 35 (30%) had TP53 AML. The median TP53 variant allele frequency was 32% (interquartile range, 16%-65%), 8 patients (23%) had only a single TP53 mutation, 15 (43%) had multiple mutations, and 12 (34%) had mutation and deletion. Outcomes were significantly worse in patients who had TP53 AML compared with those who had wild-type TP53 AML, with an overall response rate of 66% vs 89% (P = .002), a complete response/complete response with incomplete hematologic recovery rate of 57% vs 77% (P = .029), and a 60-day mortality of 26% vs 4% (P < .001), respectively. Patients with TP53 versus wild-type TP53 had shorter overall survival at 5.2 versus 19.4 months, respectively (hazard ratio, 4.67; 95% CI, 2.44-8.93; P < .0001), and shorter relapse-free survival at 3.4 versus 18.9 months (hazard ratio, 4.80; 95% CI, 1.97-11.69; P < .0001), respectively. Outcomes with DEC10-VEN in patients with TP53 AML were comparable to historical results with 10-day decitabine alone.
Patients with TP53 AML have lower response rates and shorter survival with DEC10-VEN.
TP53 突变(TP53 )在急性髓系白血病(AML)中预后不良。维奈托克联合低甲基化剂是老年患者的当前标准治疗方法;然而,最近的报告表明 TP53 对维奈托克产生耐药性。作者研究了接受 10 天阿扎胞苷和维奈托克(DEC10-VEN)治疗的 TP53 AML 患者的结局(ClinicalTrials.gov 标识符 NCT03404193)。
新诊断为 AML 的患者每 4 至 6 周接受阿扎胞苷 20 mg/m 治疗 10 天作为诱导治疗,随后在有缓解时接受 5 天阿扎胞苷治疗。维奈托克的剂量为每天 400 mg。使用下一代测序技术在骨髓样本中检测 TP53,灵敏度为 5%。根据欧洲白血病网 2017 年指南分析结局。
在 118 例患者中(中位年龄为 72 岁;年龄范围为 49-89 岁),63 例(53%)为继发性 AML,39 例(33%)为伴有复杂核型的 AML,35 例(30%)为 TP53 AML。TP53 变异等位基因频率的中位数为 32%(四分位距,16%-65%),8 例(23%)仅有单个 TP53 突变,15 例(43%)有多个突变,12 例(34%)有突变和缺失。与野生型 TP53 AML 患者相比,TP53 AML 患者的结局明显较差,总体缓解率分别为 66%和 89%(P =.002),完全缓解/完全缓解伴不完全血液学恢复率分别为 57%和 77%(P =.029),60 天死亡率分别为 26%和 4%(P <.001)。TP53 患者与野生型 TP53 患者的总生存期分别为 5.2 个月和 19.4 个月(风险比,4.67;95%CI,2.44-8.93;P <.0001),无复发生存期分别为 3.4 个月和 18.9 个月(风险比,4.80;95%CI,1.97-11.69;P <.0001)。TP53 AML 患者接受 DEC10-VEN 治疗的结局与单独使用 10 天阿扎胞苷的历史结果相当。
TP53 AML 患者接受 DEC10-VEN 治疗的缓解率较低,生存时间较短。