Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA.
Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA.
Am J Hematol. 2021 Mar 1;96(3):282-291. doi: 10.1002/ajh.26061. Epub 2020 Dec 24.
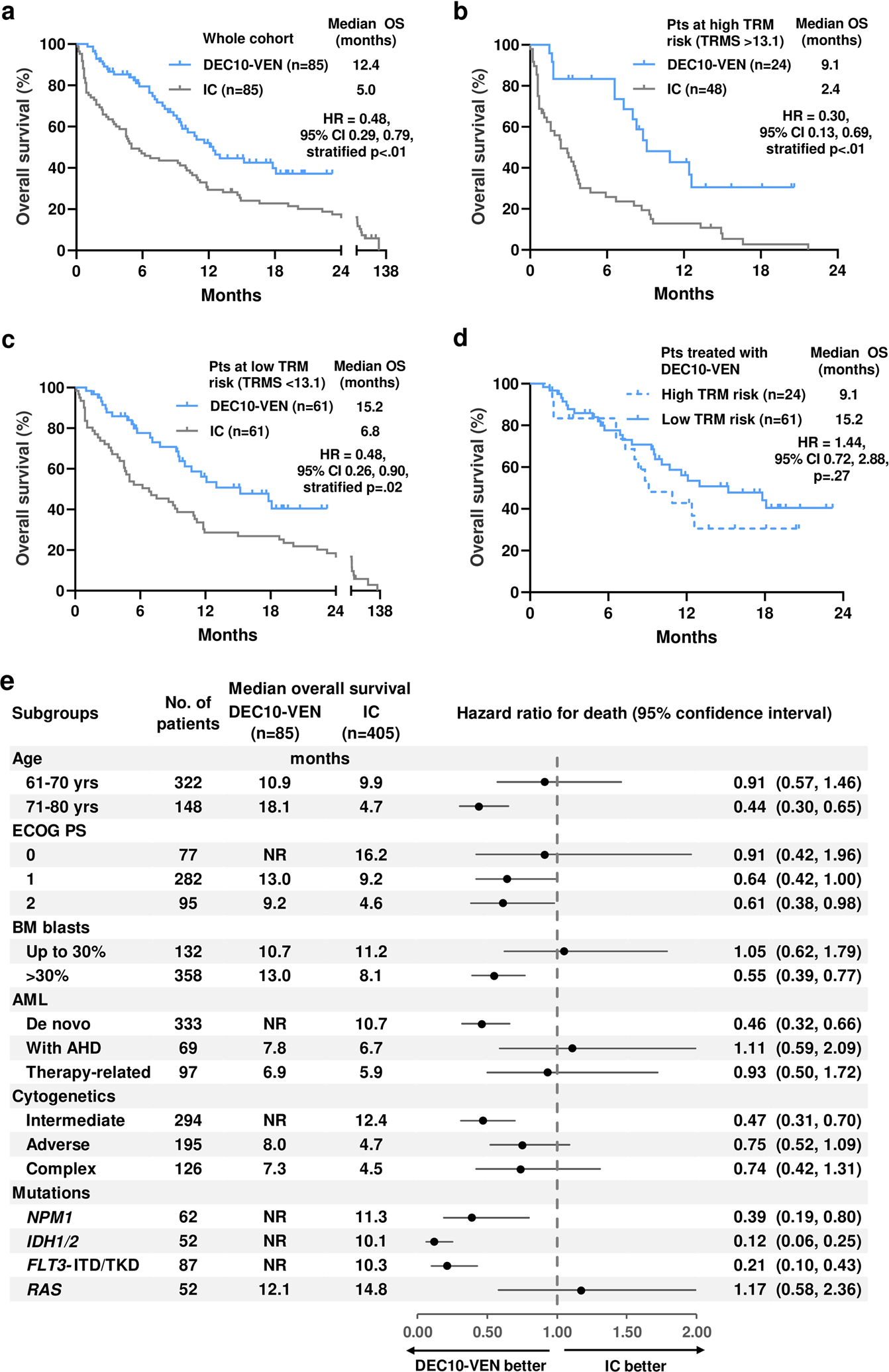
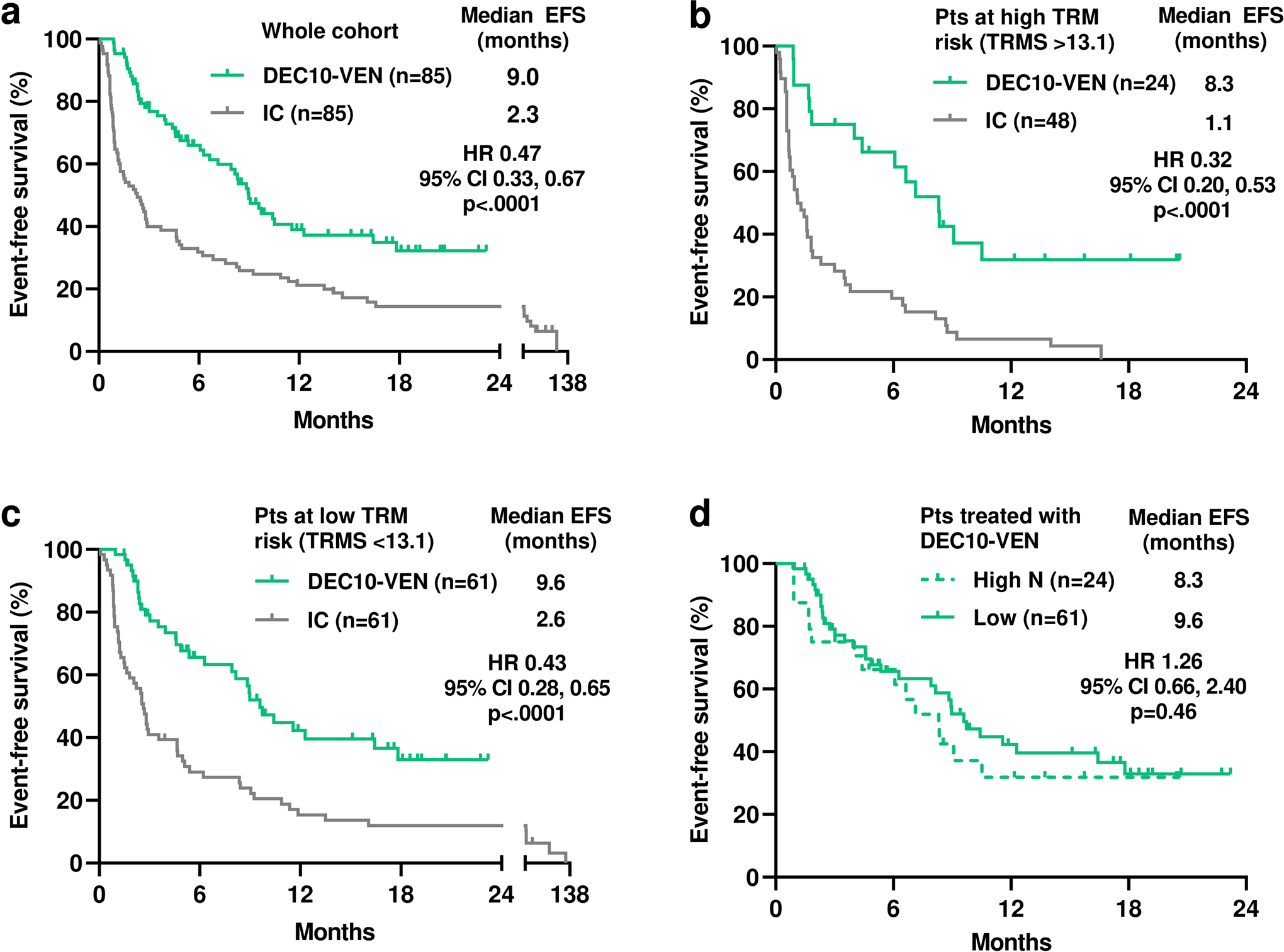
Hypomethylating agents (HMA) with venetoclax is a new standard for older/unfit patients with acute myeloid leukemia (AML). However, it is unknown how HMA with venetoclax compare to intensive chemotherapy (IC) in patients who are "fit" or "unfit" for IC. We compared outcomes of older patients with newly diagnosed AML receiving 10-day decitabine with venetoclax (DEC10-VEN) vs IC. DEC10-VEN consisted of daily venetoclax with decitabine 20 mg/m for 10 days for induction and decitabine for 5 days as consolidation. The IC cohort received regimens containing cytarabine ≥1 g/m /d. A validated treatment-related mortality score (TRMS) was used to classify patients at high-risk or low-risk for TRM with IC. Propensity scores were used to match patients to minimize bias. Median age of the DEC10-VEN cohort (n = 85) was 72 years (range 63-89) and 28% patients were at high-risk of TRM with IC. The comparator IC group (n = 85) matched closely in terms of baseline characteristics. DEC10-VEN was associated with significantly higher CR/CRi compared to IC (81% vs 52%, P < .001), and lower rate of relapse (34% vs 56%, P = .01), 30-day mortality (1% vs 24%, P < .01), and longer overall survival (OS; 12.4 vs 4.5 months, HR = 0.48, 95%CI 0.29-0.79, P < .01). In patients at both at high-risk and low-risk of TRM, DEC10-VEN showed significantly higher CR/CRi, lower 30-day mortality, and longer OS compared to IC. Patients at both high-risk and low-risk of TRM had comparable outcomes with DEC10-VEN. In conclusion, DEC10-VEN offers better outcomes compared to intensive chemotherapy in older patients with newly diagnosed AML, particularly in those at high-risk of TRM.
低甲基化药物(HMA)联合维奈托克是老年/不适合强化化疗(IC)的急性髓系白血病(AML)患者的新标准。然而,对于适合或不适合 IC 的患者,HMA 联合维奈托克与 IC 相比如何尚不清楚。我们比较了接受 10 天地西他滨联合维奈托克(DEC10-VEN)与 IC 治疗的新诊断 AML 老年患者的结局。DEC10-VEN 包括诱导期每日维奈托克联合地西他滨 20mg/m2 连用 10 天,巩固期用地西他滨连用 5 天。IC 组接受包含阿糖胞苷≥1g/m2/d 的方案。使用经过验证的治疗相关死亡率评分(TRMS)将接受 IC 的患者分为高危或低危 TRM。使用倾向评分匹配以尽量减少偏倚。DEC10-VEN 组(n=85)的中位年龄为 72 岁(范围 63-89),28%的患者接受 IC 治疗时存在 TRM 的高危风险。在基线特征方面,IC 组(n=85)与 DEC10-VEN 组匹配良好。与 IC 相比,DEC10-VEN 显著提高了完全缓解/完全缓解伴血细胞不完全恢复(CR/CRi)率(81% vs 52%,P<0.001),降低了复发率(34% vs 56%,P=0.01),30 天死亡率(1% vs 24%,P<0.01),并延长了总生存期(OS;12.4 个月 vs 4.5 个月,HR=0.48,95%CI 0.29-0.79,P<0.01)。在 TRM 高危和低危的患者中,DEC10-VEN 与 IC 相比,CR/CRi 显著更高,30 天死亡率更低,OS 更长。TRM 高危和低危的患者接受 DEC10-VEN 治疗的结局相当。总之,在新诊断 AML 的老年患者中,DEC10-VEN 提供了比强化化疗更好的结果,特别是在 TRM 高危的患者中。