Division of Gastroenterology and Hepatology, Department of Medicine, University of California-San Francisco, San Francisco, California.
Department of Epidemiology and Biostatistics, University of California-San Francisco, San Francisco, California; Division of General Internal Medicine, Department of Medicine, University of California-San Francisco, San Francisco, California.
Gastroenterology. 2021 Nov;161(5):1487-1501.e5. doi: 10.1053/j.gastro.2021.07.010. Epub 2021 Jul 18.
BACKGROUND & AIMS: In patients with chronic liver disease (CLD) with or without cirrhosis, existing studies on the outcomes with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection have limited generalizability. We used the National COVID Cohort Collaborative (N3C), a harmonized electronic health record dataset of 6.4 million, to describe SARS-CoV-2 outcomes in patients with CLD and cirrhosis.
We identified all patients with CLD with or without cirrhosis who had SARS-CoV-2 testing in the N3C Data Enclave as of July 1, 2021. We used survival analyses to associate SARS-CoV-2 infection, presence of cirrhosis, and clinical factors with the primary outcome of 30-day mortality.
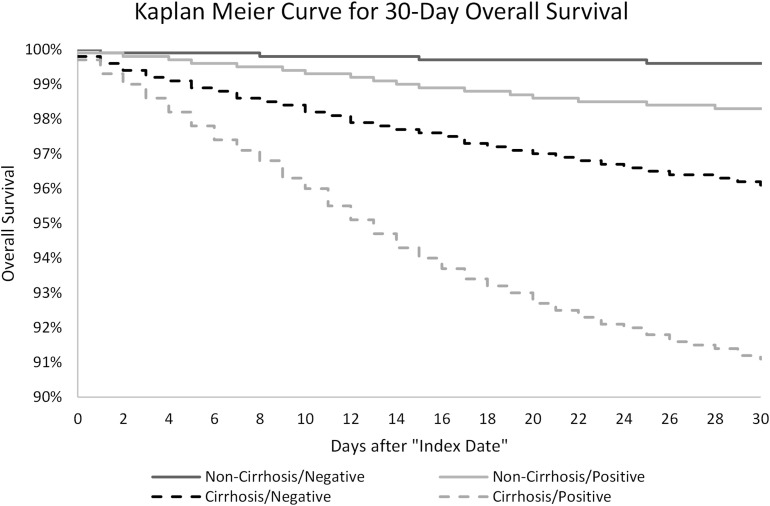
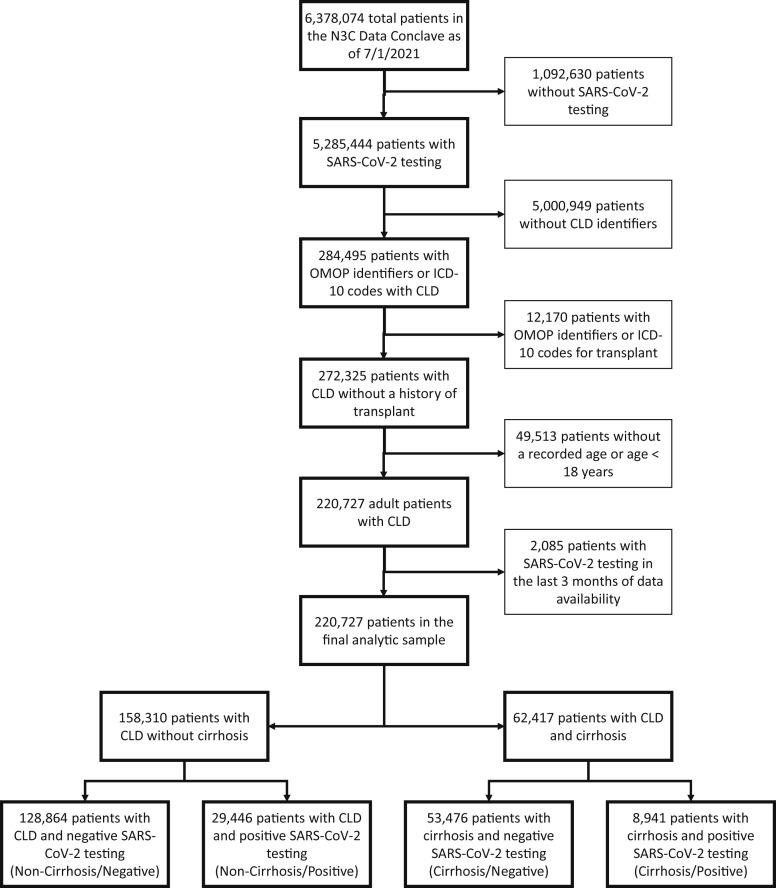
We isolated 220,727 patients with CLD and SARS-CoV-2 test status: 128,864 (58%) were noncirrhosis/negative, 29,446 (13%) were noncirrhosis/positive, 53,476 (24%) were cirrhosis/negative, and 8941 (4%) were cirrhosis/positive patients. Thirty-day all-cause mortality rates were 3.9% in cirrhosis/negative and 8.9% in cirrhosis/positive patients. Compared to cirrhosis/negative patients, cirrhosis/positive patients had 2.38 times adjusted hazard of death at 30 days. Compared to noncirrhosis/positive patients, cirrhosis/positive patients had 3.31 times adjusted hazard of death at 30 days. In stratified analyses among patients with cirrhosis with increased age, obesity, and comorbid conditions (ie, diabetes, heart failure, and pulmonary disease), SARS-CoV-2 infection was associated with increased adjusted hazard of death.
In this study of approximately 221,000 nationally representative, diverse, and sex-balanced patients with CLD; we found SARS-CoV-2 infection in patients with cirrhosis was associated with 2.38 times mortality hazard, and the presence of cirrhosis among patients with CLD infected with SARS-CoV-2 was associated with 3.31 times mortality hazard. These results provide an additional impetus for increasing vaccination uptake and further research regarding immune responses to vaccines in patients with severe liver disease.
在患有慢性肝病(CLD)的患者中,无论是否存在肝硬化,现有关于严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)感染结果的研究具有一定的局限性。我们使用了国家 COVID 队列协作(N3C),这是一个由 640 万电子健康记录组成的协调数据集,来描述肝硬化患者中 SARS-CoV-2 的结果。
我们在 N3C 数据飞地中确定了截至 2021 年 7 月 1 日患有 CLD 且有 SARS-CoV-2 检测的所有患者。我们使用生存分析将 SARS-CoV-2 感染、肝硬化的存在以及临床因素与 30 天死亡率的主要结局相关联。
我们分离出了 220727 名患有 CLD 且有 SARS-CoV-2 检测的患者:128864 名(58%)为非肝硬化/阴性,29446 名(13%)为非肝硬化/阳性,53476 名(24%)为肝硬化/阴性,8941 名(4%)为肝硬化/阳性。肝硬化/阴性患者的 30 天全因死亡率为 3.9%,肝硬化/阳性患者的 30 天全因死亡率为 8.9%。与肝硬化/阴性患者相比,肝硬化/阳性患者在 30 天时有 2.38 倍的死亡调整危险比。与非肝硬化/阳性患者相比,肝硬化/阳性患者在 30 天时的死亡调整危险比为 3.31 倍。在肝硬化患者中,分层分析显示年龄较大、肥胖和合并症(即糖尿病、心力衰竭和肺部疾病)的患者中,SARS-CoV-2 感染与调整后的死亡危险增加相关。
在这项大约 221000 名全国代表性、多样化且性别平衡的患有 CLD 的患者的研究中,我们发现肝硬化患者中 SARS-CoV-2 感染与 2.38 倍的死亡率危险比相关,而在感染 SARS-CoV-2 的 CLD 患者中存在肝硬化与 3.31 倍的死亡率危险比相关。这些结果为增加疫苗接种率提供了额外的动力,并进一步推动了对严重肝病患者疫苗免疫反应的研究。