Liaison Psychiatry Unit, 1 Place de l'Hopital, University Hospitals Strasbourg, Strasbourg, France.
Academic Neurology Unit, Royal Hallamshire Hospital, The University of Sheffield, Sheffield, UK.
Epilepsia Open. 2021 Sep;6(3):472-482. doi: 10.1002/epi4.12521. Epub 2021 Jul 31.
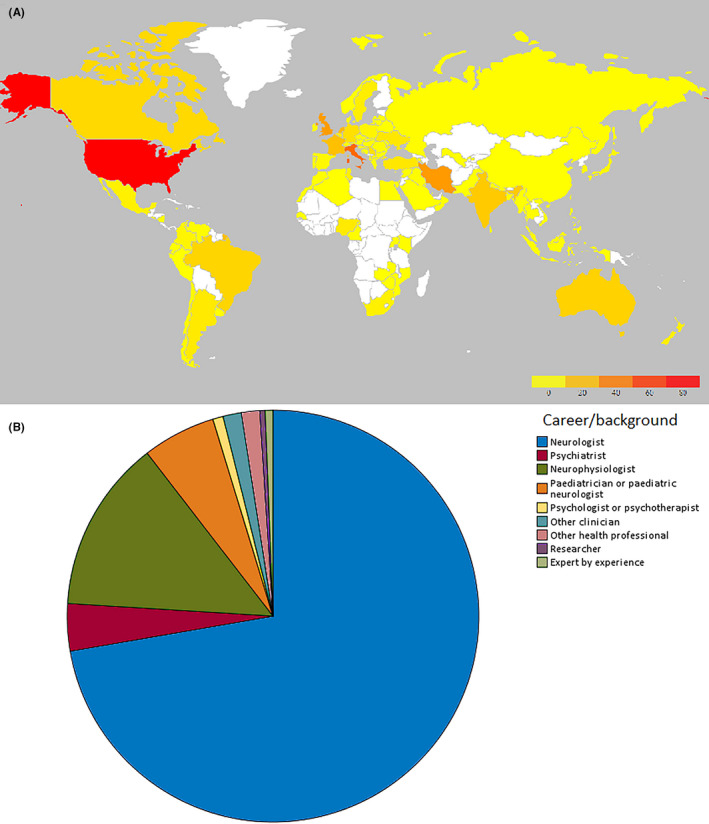
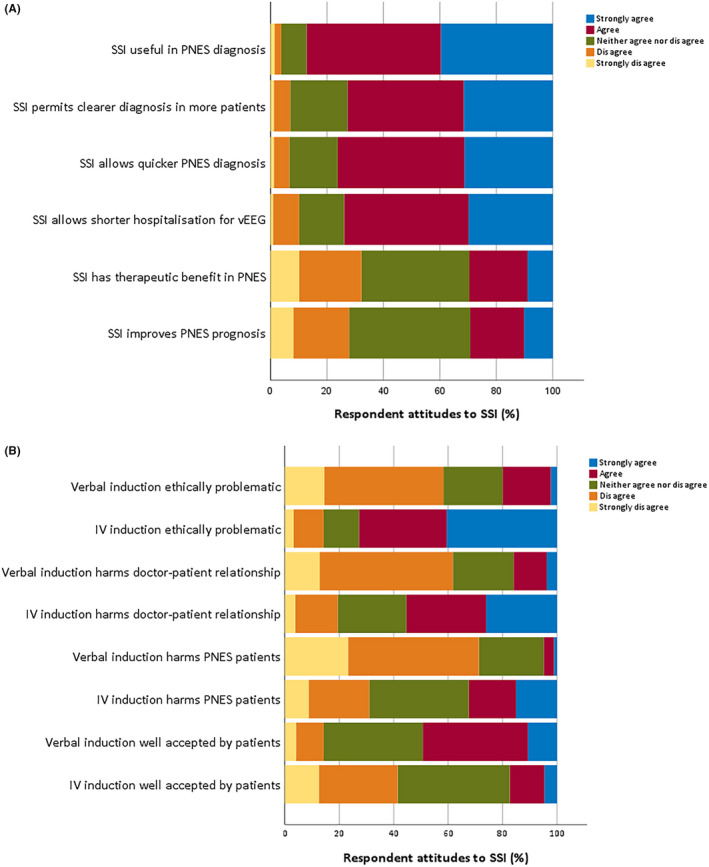
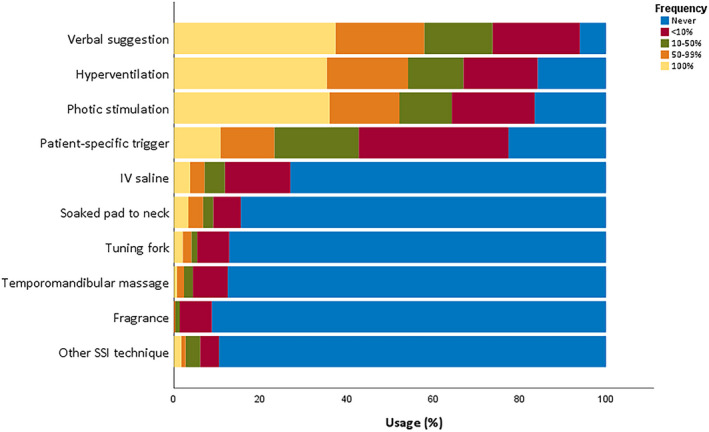
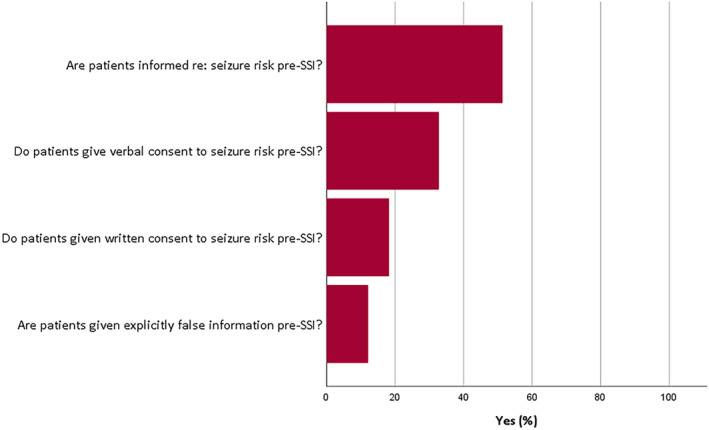
Video-encephalographic (vEEG) seizure recordings make essential contributions to the differentiation of epilepsy and psychogenic nonepileptic seizures (PNES). The yield of vEEG examinations can be increased through suggestive seizure manipulation (SSM) (ie, activation/provocation/cessation procedures), but its use has raised ethical concerns. In preparation for guidelines on the investigation of patients with PNES, the ILAE PNES Task Force carried out an international survey to investigate practices of and opinions about SSM. An online questionnaire was developed by the ILAE PNES Task Force. Questions were asked at clinical unit or individual respondent level. All ILAE chapters were encouraged to send questionnaires to their members. The survey was open from July 1, 2019, to August 31, 2019. A total of 487 clinicians from 411 units across 94 countries responded. Some form of SSM was used in 296/411 units (72.0%). Over 90% reported the use of verbal suggestion, over 80% the use of activation procedures also capable of eliciting epileptic activity (hyperventilation or photic stimulation). Only 26.3% of units used techniques specifically intended to provoke PNES (eg, saline injection). Fewer than 10% of units had established protocols for SSM, only 20% of units required written patient consent, in 12.2% of units patients received explicitly false information to provoke seizures. Clinicians using SSM tended to perceive no ethical problems, whereas those not using SSM were likely to have ethical concerns about these methods. We conclude that the use of invasive nocebo techniques intended to provoke PNES in diagnostic settings has declined, but SSM is commonly combined with activation procedures also capable of eliciting epileptic activity. While research suggests that openness about the use of PNES-specific nocebo techniques does not reduce diagnostic yield, very few units have suggestion protocols or seek patient consent. This could be addressed through establishing consensus guidance for the practice of SSM.
视频脑电图(vEEG)癫痫发作记录对癫痫和心因性非癫痫性发作(PNES)的鉴别诊断具有重要意义。通过暗示性发作操作(SSM)(即激活/激发/停止程序)可以提高 vEEG 检查的检出率,但它的使用引起了伦理问题。为了制定 PNES 患者的调查指南,ILAE PNES 工作组进行了一项国际调查,以调查 SSM 的实践和意见。ILAE PNES 工作组制定了一份在线问卷。问题是在临床单位或个人回答者层面提出的。鼓励所有 ILAE 分会向其成员发送问卷。该调查于 2019 年 7 月 1 日至 2019 年 8 月 31 日开放。来自 94 个国家的 411 个单位的 487 名临床医生做出了回应。296/411 个单位(72.0%)采用了某种形式的 SSM。超过 90%的单位报告使用口头建议,超过 80%的单位使用也能引起癫痫活动的激活程序(过度通气或光刺激)。只有 26.3%的单位使用专门用于引发 PNES 的技术(例如,生理盐水注射)。不到 10%的单位制定了 SSM 的方案,只有 20%的单位要求书面患者同意,在 12.2%的单位中,患者接受了明确的虚假信息来引发发作。使用 SSM 的临床医生往往认为没有伦理问题,而不使用 SSM 的临床医生则可能对这些方法存在伦理问题。我们的结论是,在诊断环境中有意使用侵入性的 PNES 特定的厌恶技术的情况有所减少,但 SSM 通常与也能引发癫痫活动的激活程序相结合。虽然研究表明,公开使用特定于 PNES 的厌恶技术不会降低诊断率,但很少有单位有建议方案或寻求患者同意。通过制定 SSM 实践的共识指南,可以解决这个问题。