Applied Design, Cape Peninsula University of Technology, Bellville, South Africa
Open Heart. 2021 Jul;8(2). doi: 10.1136/openhrt-2021-001680.
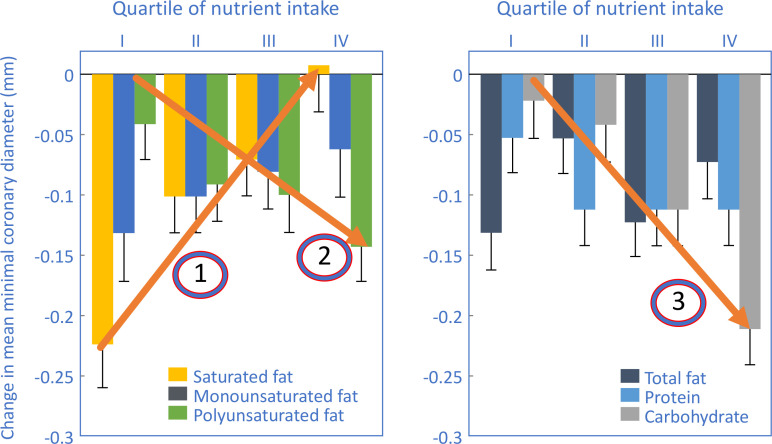
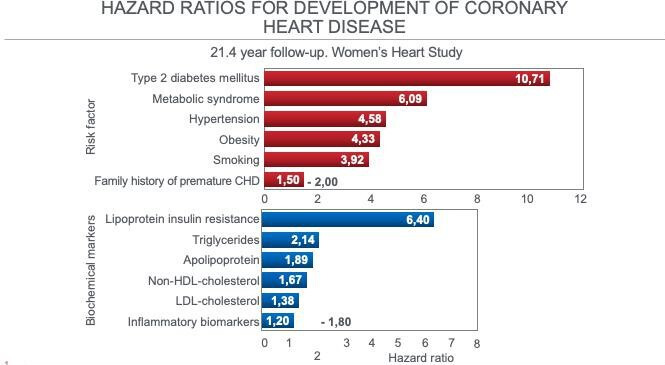
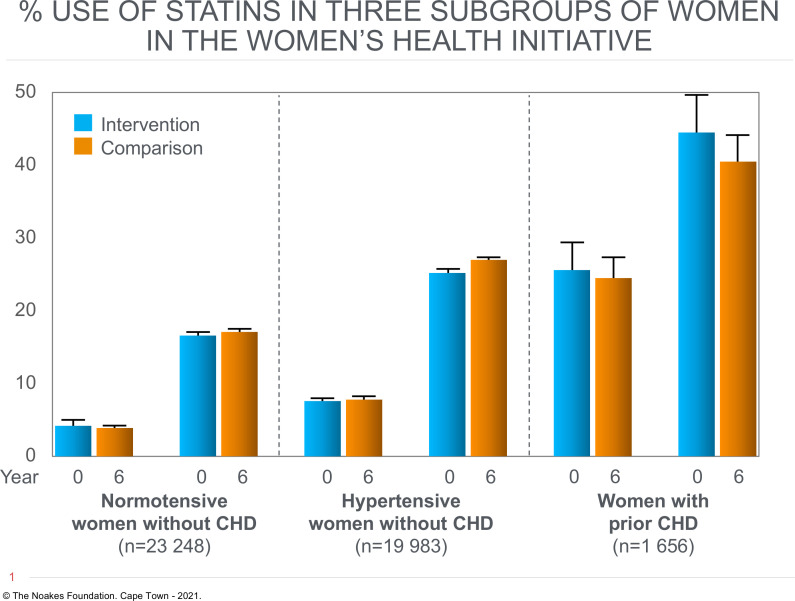
The Women's Health Initiative Randomized Controlled Dietary Modification Trial (WHIRCDMT) was designed to test whether the US Department of Agriculture's 1977 Dietary Guidelines for Americans protects against coronary heart disease (CHD) and other chronic diseases. The only significant finding in the original 2006 WHIRCDMT publication was that postmenopausal women with CHD randomised to a low-fat 'heart-healthy' diet in 1993 were at 26% greater risk of developing additional CHD events compared with women with CHD eating the control diet. A 2017 WHIRCDMT publication includes data for an additional 5 years of follow-up. It finds that CHD risk in this subgroup of postmenopausal women had increased further to 47%-61%. The authors present three post-hoc rationalisations to explain why this finding is 'inadmissible': (1) only women in this subgroup were less likely to adhere to the prescribed dietary intervention; (2) their failure to follow the intervention diet increased their CHD risk; and (3) only these women were more likely to not have received cholesterol-lowering drugs. These rationalisations appear spurious. Rather these findings are better explained as a direct consequence of postmenopausal women with features of insulin resistance (IR) eating a low-fat high-carbohydrate diet for 13 years. All the worst clinical features of IR, including type 2 diabetes mellitus (T2DM) in some, can be 'reversed' by the prescription of a high-fat low-carbohydrate diet. The Women's Health Study has recently reported that T2DM (10.71-fold increased risk) and other markers of IR including metabolic syndrome (6.09-fold increased risk) were the most powerful predictors of future CHD development in women; blood low-density lipoprotein-cholesterol concentration was a poor predictor (1.38-fold increased risk). These studies challenge the prescription of the low-fat high-carbohydrate heart-healthy diet, at least in postmenopausal women with IR, especially T2DM. According to the medical principle of 'first do no harm', this practice is now shown to be evidence-based, making it scientifically unjustifiable, perhaps unethical.
妇女健康倡议随机对照饮食修正试验(WHIRCDMT)旨在测试美国农业部 1977 年的《美国人饮食指南》是否能预防冠心病(CHD)和其他慢性病。最初的 2006 年 WHIRCDMT 出版物中唯一一项重要发现是,1993 年被随机分配到低脂“心脏健康”饮食的患有 CHD 的绝经后妇女,与食用对照饮食的患有 CHD 的妇女相比,发生其他 CHD 事件的风险增加了 26%。2017 年 WHIRCDMT 出版物包含了另外 5 年的随访数据。研究发现,该亚组绝经后妇女的 CHD 风险进一步增加了 47%-61%。作者提出了三个事后合理化解释,说明为什么这一发现是“不可接受的”:(1)只有这个亚组的女性更不可能坚持规定的饮食干预;(2)她们没有遵循干预饮食,增加了 CHD 风险;(3)只有这些女性更不可能服用降胆固醇药物。这些合理化解释似乎是没有根据的。相反,这些发现可以更好地解释为具有胰岛素抵抗(IR)特征的绝经后妇女 13 年来食用低脂高碳水化合物饮食的直接后果。IR 的所有最坏的临床特征,包括一些人的 2 型糖尿病(T2DM),都可以通过开高脂肪低碳水化合物饮食来“逆转”。《女性健康研究》最近报告称,T2DM(风险增加 10.71 倍)和其他 IR 标志物,包括代谢综合征(风险增加 6.09 倍),是女性未来 CHD 发展的最强预测因素;血液低密度脂蛋白胆固醇浓度是一个较差的预测因素(风险增加 1.38 倍)。这些研究挑战了低脂高碳水化合物心脏健康饮食的处方,至少在具有 IR 的绝经后妇女中,尤其是 T2DM 患者。根据“首先不造成伤害”的医学原则,这种做法现在被证明是有证据的,因此在科学上是不合理的,也许是不道德的。