The Intervention Centre, Rikshospitalet, Oslo University Hospital, Oslo, Norway.
Division of Emergencies and Critical Care, Department of Research and Development, Oslo University Hospital, Oslo, Norway.
Ann Surg Oncol. 2022 Jan;29(1):366-375. doi: 10.1245/s10434-021-10464-6. Epub 2021 Jul 22.
Resection margin status is considered one of the few surgeon-controlled parameters affecting prognosis in pancreatic ductal adenocarcinoma (PDAC). While studies mostly focus on resection margins in pancreatoduodenectomy, little is known about their role in distal pancreatectomy (DP). This study aimed to investigate resection margins in DP for PDAC.
Patients who underwent DP for PDAC between October 2004 and February 2020 were included (n = 124). Resection margins and associated parameters were studied in two consecutive time periods during which different pathology examination protocols were used: non-standardized (period 1: 2004-2014) and standardized (period 2: 2015-2020). Microscopic margin involvement (R1) was defined as ≤1 mm clearance.
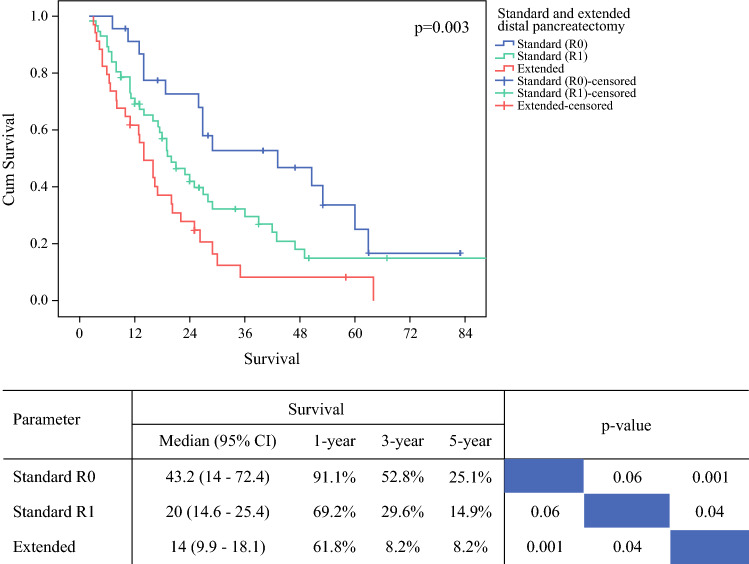
Laparoscopic and open resections were performed in 117 (94.4%) and 7 (5.6%) patients, respectively. The R1 rate for the entire cohort was 73.4%, increasing from 60.4% in period 1 to 83.1% in period 2 (p = 0.005). A significantly higher R1 rate was observed for the posterior margin (35.8 vs. 70.4%, p < 0.001) and anterior pancreatic surface (based on a 0 mm clearance; 18.9 vs. 35.4%, p = 0.045). Pathology examination period, poorly differentiated PDAC, and vascular invasion were associated with R1 in the multivariable model. Extended DP, positive anterior pancreatic surface, lymph node ratio, perineural invasion, and adjuvant chemotherapy, but not R1, were significant prognostic factors for overall survival in the entire cohort.
Pathology examination is a key determinant of resection margin status following DP for PDAC. A high R1 rate is to be expected when pathology examination is meticulous and standardized. Involvement of the anterior pancreatic surface affects prognosis.
在胰腺导管腺癌 (PDAC) 中,切缘状态被认为是少数几个受外科医生控制的影响预后的参数之一。虽然大多数研究都集中在胰十二指肠切除术的切缘,但对远端胰腺切除术 (DP) 中的切缘作用知之甚少。本研究旨在研究 DP 治疗 PDAC 的切缘。
纳入 2004 年 10 月至 2020 年 2 月期间接受 DP 治疗 PDAC 的患者(n=124)。研究了在两个连续的时间段内 DP 的切缘及相关参数,在此期间使用了不同的病理检查方案:非标准化(第一阶段:2004-2014 年)和标准化(第二阶段:2015-2020 年)。定义显微镜下切缘受累(R1)为≤1mm 间隙。
分别有 117 例(94.4%)和 7 例(5.6%)患者接受了腹腔镜和开放性手术。整个队列的 R1 率为 73.4%,第一阶段为 60.4%,第二阶段为 83.1%(p=0.005)。后缘(35.8%比 70.4%,p<0.001)和前胰腺表面(以 0mm 间隙为基础;18.9%比 35.4%,p=0.045)的 R1 率明显更高。多变量模型中,病理检查期、分化差的 PDAC 和血管侵犯与 R1 相关。在整个队列中,广泛 DP、前胰腺表面阳性、淋巴结比率、神经周围侵犯和辅助化疗是总生存的显著预后因素,而不是 R1。
病理检查是 DP 治疗 PDAC 后切缘状态的关键决定因素。当病理检查细致且标准化时,预计 R1 率会很高。前胰腺表面受累会影响预后。