The Ohio State University Wexner Medical Center, Division of Cardiovascular Medicine, Columbus.
Duke Clinical Research Institute, Duke University School of Medicine, Durham, North Carolina.
JAMA Netw Open. 2021 Jul 1;4(7):e2117963. doi: 10.1001/jamanetworkopen.2021.17963.
Randomized clinical trials (RCTs) are critical in advancing patient care, yet conducting such large-scale trials requires tremendous resources and coordination. Clinical site start-up performance metrics can provide insight into opportunities for improved trial efficiency but have not been well described.
To measure the start-up time needed to reach prespecified milestones across sites in large cardiovascular RCTs in North America and to evaluate how these metrics vary by time and type of regulatory review process.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study evaluated cardiovascular RCTs conducted from July 13, 2004, to February 1, 2017. The RCTs were coordinated by a single academic research organization, the Duke Clinical Research Institute. Nine consecutive trials with completed enrollment and publication of results in their target journal were studied. Data were analyzed from December 4, 2019, to January 11, 2021.
Year of trial enrollment initiation (2004-2007 vs 2008-2012) and use of a central vs local institutional review board (IRB).
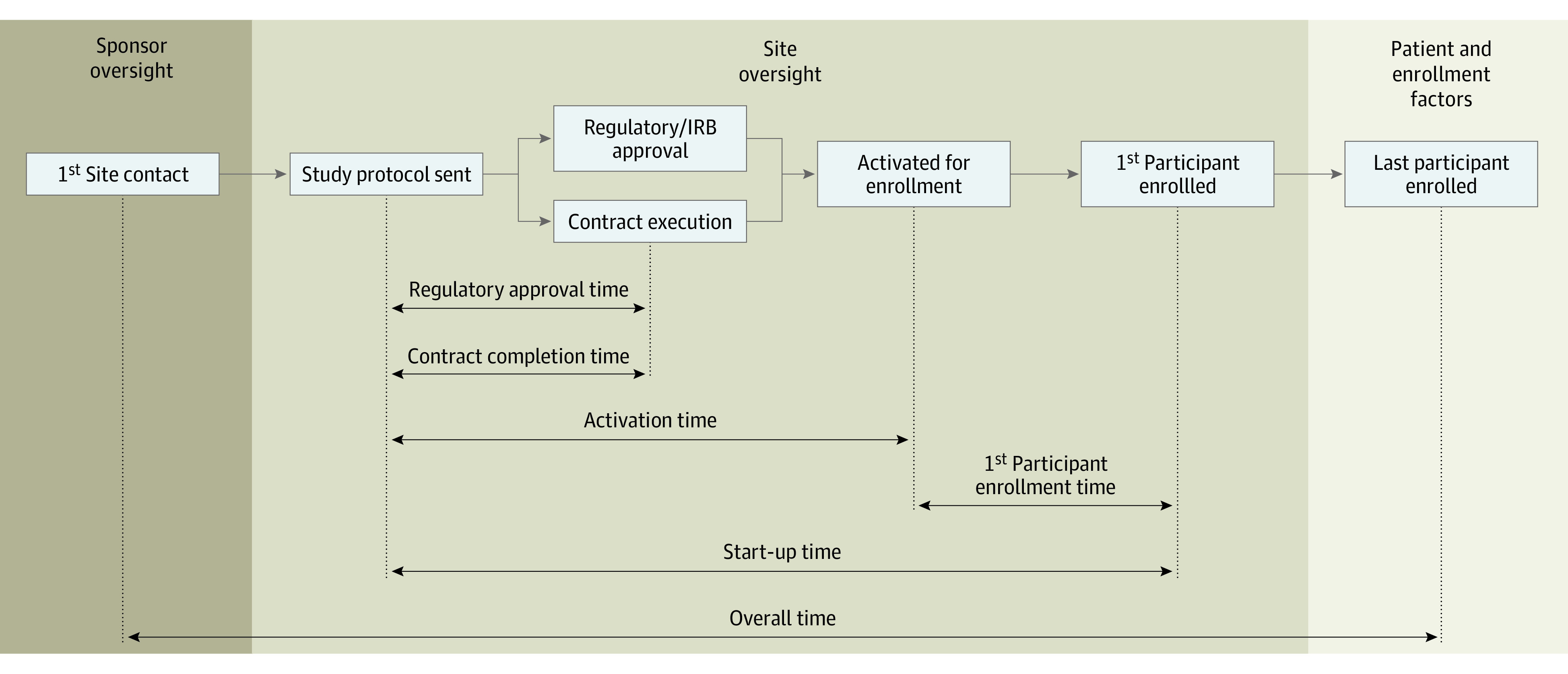
The primary outcome was the median start-up time (from study protocol delivery to first participant enrollment) as compared by trial year and type of IRB used. The median start-up time for the top 10% of sites was also reported. Secondary outcomes included time to site regulatory approval, time to contract execution, and time to site activation.
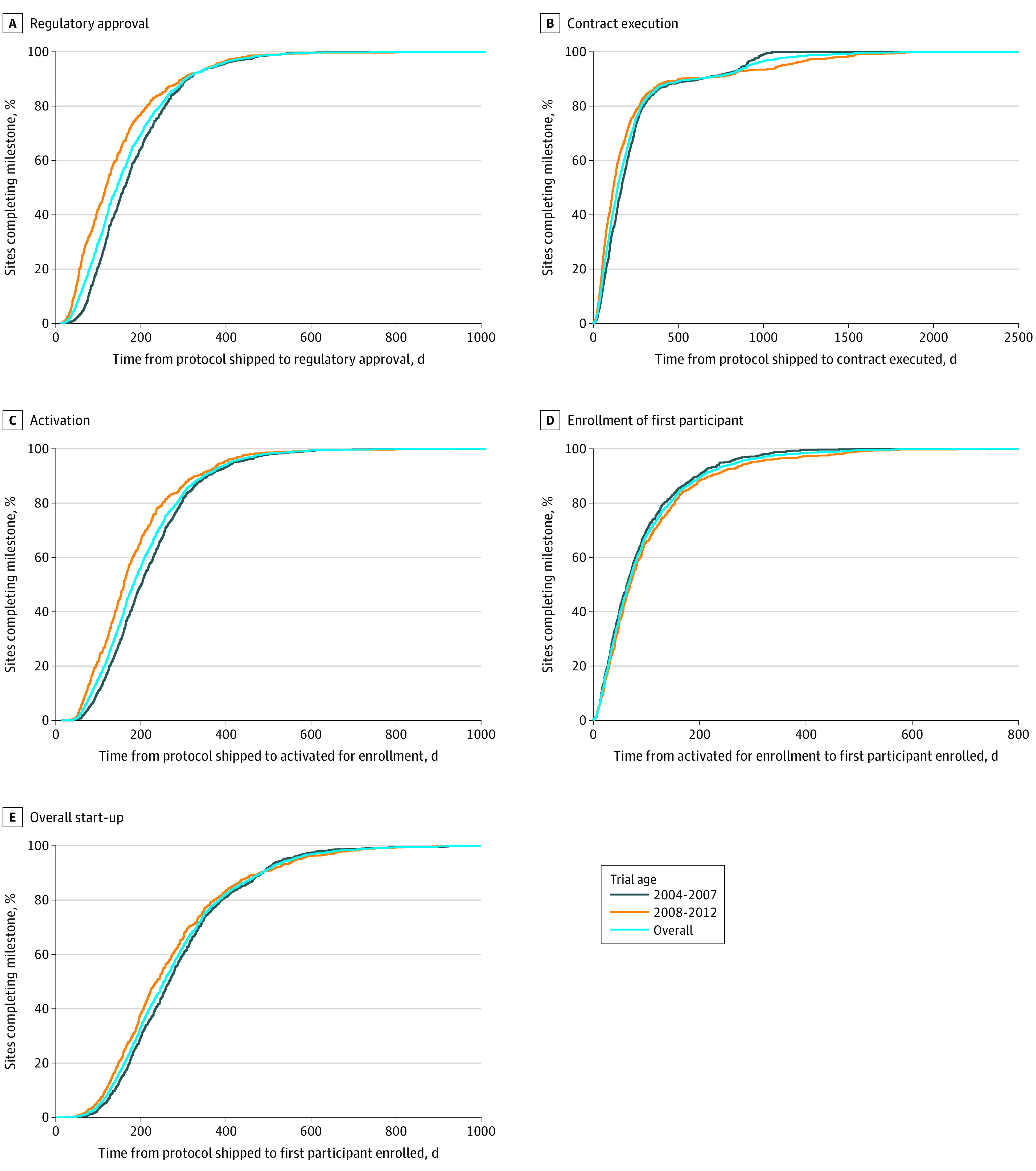
For the 9 RCTs included, the median site start-up time shortened only slightly over time from 267 days (interquartile range [IQR], 185-358 days) for 2004-2007 trials to 237 days (IQR, 162-343 days) for 2008-2012 trials (overall median, 255 days [IQR, 177-350 days]; P < .001). For the top 10% of sites, median start-up time was 107 days (IQR, 95-121 days) for 2004-2007 trials vs 104 days (IQR, 84-118 days) for 2008-2012 trials (overall median, 106 days [IQR, 90-120 days]; P = .04). The median start-up time was shorter among sites using a central IRB (199 days [IQR, 140-292 days]) than those using a local IRB (287 days [IQR, 205-390 days]; P < .001).
This cohort study of North American research sites in large cardiovascular RCTs found a duration of nearly 9 months from the time of study protocol delivery to the first participant enrollment; this metric was only slightly shortened during the study period but was reduced to less than 4 months for top-performing sites. These findings suggest that the use of central IRBs has the potential to improve RCT efficiency.
随机临床试验 (RCT) 对推进患者护理至关重要,但进行如此大规模的试验需要巨大的资源和协调。临床站点启动性能指标可以深入了解提高试验效率的机会,但尚未得到很好的描述。
测量在北美的大型心血管 RCT 中,各站点达到预定里程碑所需的启动时间,并评估这些指标如何随时间和监管审查过程的类型而变化。
设计、设置和参与者:这项队列研究评估了 2004 年 7 月 13 日至 2017 年 2 月 1 日进行的心血管 RCT。这些 RCT 由一个名为杜克临床研究所的单一学术研究组织协调。研究了九项连续的试验,这些试验已完成入组并在其目标期刊上发表了结果。数据于 2019 年 12 月 4 日至 2021 年 1 月 11 日进行分析。
试验入组启动年份(2004-2007 年与 2008-2012 年)和使用中央与当地机构审查委员会(IRB)。
主要结果是比较试验年份和使用的 IRB 类型的中位数启动时间(从研究方案交付到第一个参与者入组)。还报告了前 10%的站点的中位数启动时间。次要结果包括站点监管批准时间、合同执行时间和站点激活时间。
在纳入的 9 项 RCT 中,站点启动时间仅略有缩短,从 2004-2007 年试验的 267 天(四分位距 [IQR],185-358 天)缩短至 2008-2012 年试验的 237 天(IQR,162-343 天)(总体中位数,255 天 [IQR,177-350 天];P < .001)。对于前 10%的站点,2004-2007 年试验的中位数启动时间为 107 天(IQR,95-121 天),而 2008-2012 年试验的中位数启动时间为 104 天(IQR,84-118 天)(总体中位数,106 天 [IQR,90-120 天];P = .04)。使用中央 IRB 的站点的中位数启动时间(199 天 [IQR,140-292 天])短于使用当地 IRB 的站点(287 天 [IQR,205-390 天];P < .001)。
这项对北美的大型心血管 RCT 研究站点的队列研究发现,从研究方案交付到第一个参与者入组的时间长达近 9 个月;在研究期间,这一指标略有缩短,但对于表现最好的站点,这一指标缩短到不到 4 个月。这些发现表明,使用中央 IRB 有可能提高 RCT 效率。