Department of Epidemiology, Fairbanks School of Public Health, Indiana University, Bloomington, Indiana, United States of America.
Center for Biomedical Informatics, Regenstrief Institute, Indianapolis, Indiana, United States of America.
PLoS One. 2021 Jul 23;16(7):e0255063. doi: 10.1371/journal.pone.0255063. eCollection 2021.
Early studies on COVID-19 identified unequal patterns in hospitalization and mortality in urban environments for racial and ethnic minorities. These studies were primarily single center observational studies conducted within the first few weeks or months of the pandemic. We sought to examine trends in COVID-19 morbidity, hospitalization, and mortality over time for minority and rural populations, especially during the U.S. fall surge.
Data were extracted from a statewide cohort of all adult residents in Indiana tested for SARS-CoV-2 infection between March 1 and December 31, 2020, linked to electronic health records. Primary measures were per capita rates of infection, hospitalization, and death. Age adjusted rates were calculated for multiple time periods corresponding to public health mitigation efforts. Comparisons across time within groups were compared using ANOVA.
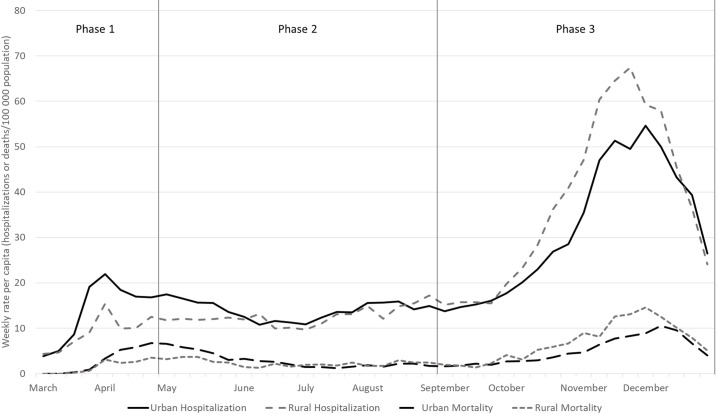
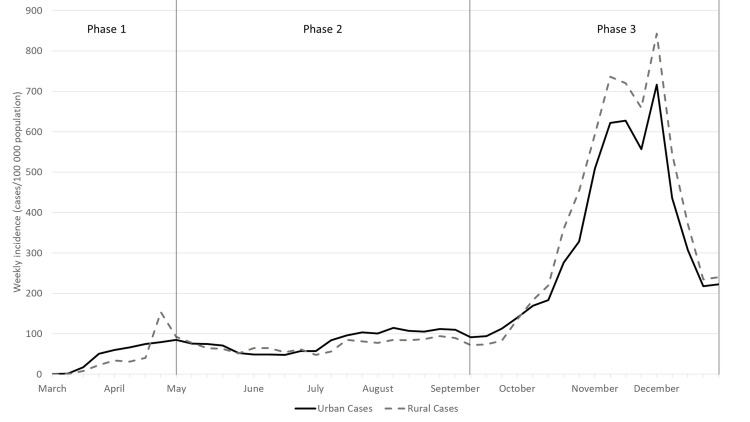
Morbidity and mortality increased over time with notable differences among sub-populations. Initially, hospitalization rates among racial minorities were 3-4 times higher than whites, and mortality rates among urban residents were twice those of rural residents. By fall 2020, hospitalization and mortality rates in rural areas surpassed those of urban areas, and gaps between black/brown and white populations narrowed. Changes across time among demographic groups was significant for morbidity and hospitalization. Cumulative morbidity and mortality were highest among minority groups and in rural communities.
The synchronicity of disparities in COVID-19 by race and geography suggests that health officials should explicitly measure disparities and adjust mitigation as well as vaccination strategies to protect those sub-populations with greater disease burden.
早期关于 COVID-19 的研究发现,在城市环境中,少数族裔和种族的住院和死亡率存在不平等模式。这些研究主要是在大流行的最初几周或几个月内进行的单中心观察性研究。我们试图研究少数民族和农村人口 COVID-19 发病率、住院率和死亡率随时间的变化趋势,特别是在美国秋季激增期间。
从印第安纳州全州范围内的所有成年居民队列中提取数据,这些居民在 2020 年 3 月 1 日至 12 月 31 日期间接受了 SARS-CoV-2 感染检测,并与电子健康记录相关联。主要措施是每千人感染、住院和死亡的比例。对于与公共卫生缓解措施相对应的多个时间段,计算了年龄调整后的比率。使用方差分析比较组内随时间的比较。
发病率和死亡率随时间增加,不同亚群之间存在显著差异。最初,少数族裔的住院率是白人的 3-4 倍,城市居民的死亡率是农村居民的两倍。到 2020 年秋季,农村地区的住院和死亡率超过了城市地区,黑人和棕色人种与白人之间的差距缩小。不同时间内人口群体之间的变化在发病率和住院率方面具有统计学意义。少数民族和农村社区的累积发病率和死亡率最高。
COVID-19 在种族和地理位置上的差异具有同步性,这表明卫生官员应该明确衡量差异,并调整缓解和疫苗接种策略,以保护那些疾病负担更大的亚人群。