Kato Yoko, Kizer Jorge R, Ostovaneh Mohammad R, Lazar Jason, Peng Qi, van der Geest Rob J, Lima Joao A C, Ambale-Venkatesh Bharath
Department of Cardiology, Johns Hopkins University, Baltimore, MD, USA.
Cardiology Section, San Francisco Veterans Affairs Health Care System, and Departments of Medicine, Epidemiology and Biostatistics, University of California San Francisco, San Francisco, CA, USA.
BMC Med Imaging. 2021 Jul 27;21(1):116. doi: 10.1186/s12880-021-00649-6.
Quantification of non-ischemic myocardial scar remains a challenge due to the patchy diffuse nature of fibrosis. Extracellular volume (ECV) to guide late gadolinium enhancement (LGE) analysis may achieve a robust scar assessment.
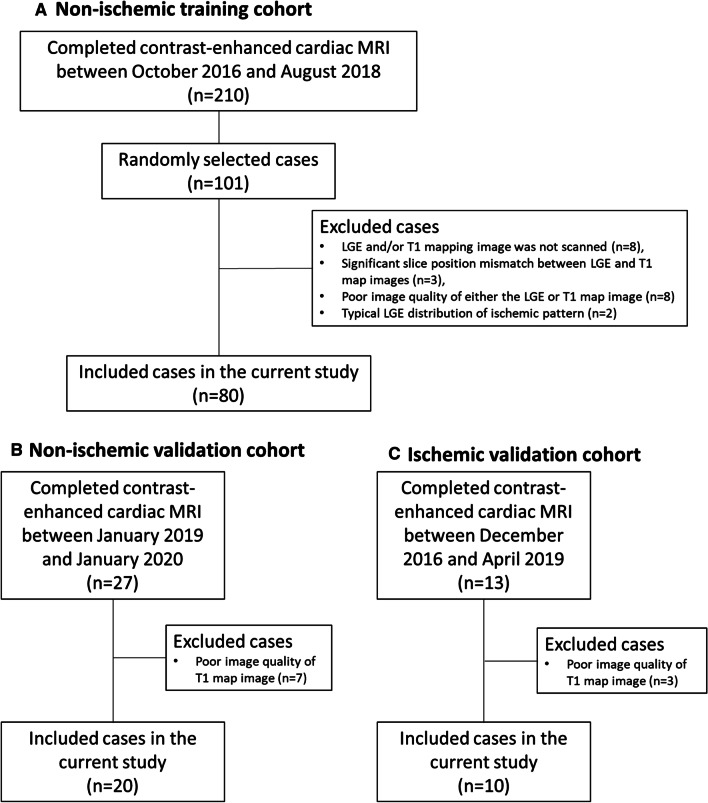
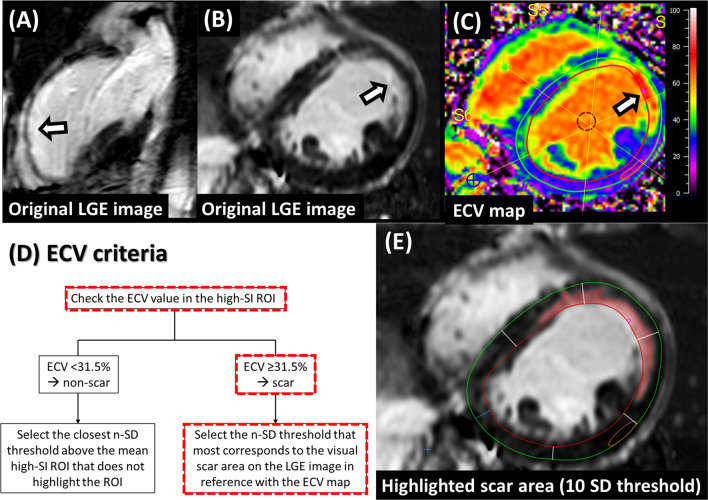
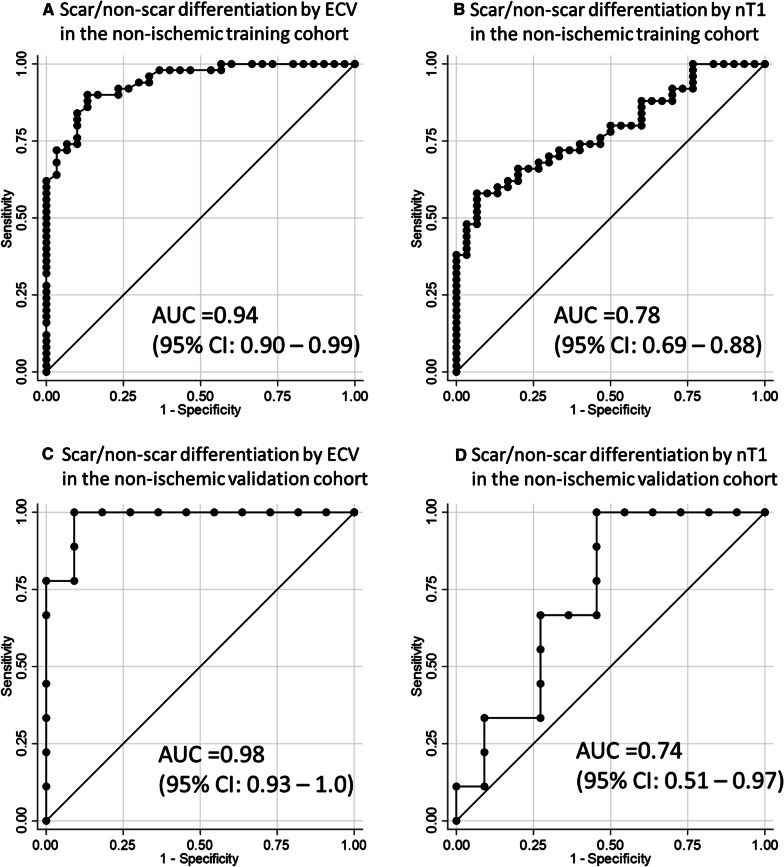
Three cohorts of 80 non-ischemic-training, 20 non-ischemic-validation, and 10 ischemic-validation were prospectively enrolled and underwent 3.0 Tesla cardiac MRI. An ECV cutoff to differentiate LGE scar from non-scar was identified in the training cohort from the receiver-operating characteristic curve analysis, by comparing the ECV value against the visually-determined presence/absence of the LGE scar at the highest signal intensity (SI) area of the mid-left ventricle (LV) LGE. Based on the ECV cutoff, an LGE semi-automatic threshold of n-times of standard-deviation (n-SD) above the remote-myocardium SI was optimized in the individual cases ensuring correspondence between LGE and ECV images. The inter-method agreement of scar amount in comparison with manual (for non-ischemic) or full-width half-maximum (FWHM, for ischemic) was assessed. Intra- and inter-observer reproducibility were investigated in a randomly chosen subset of 40 non-ischemic and 10 ischemic cases.
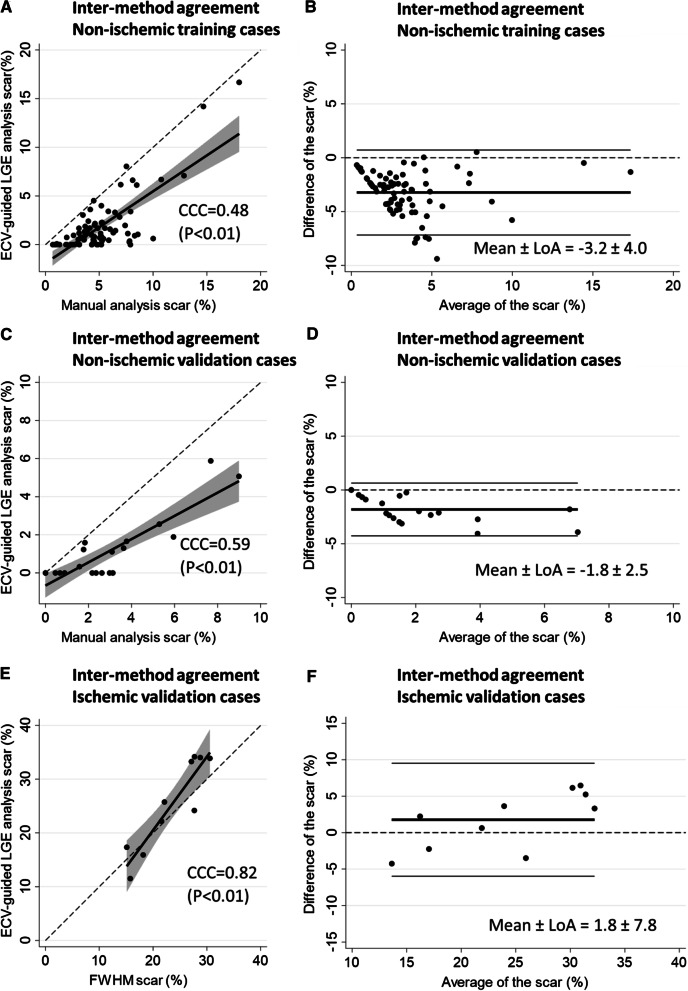
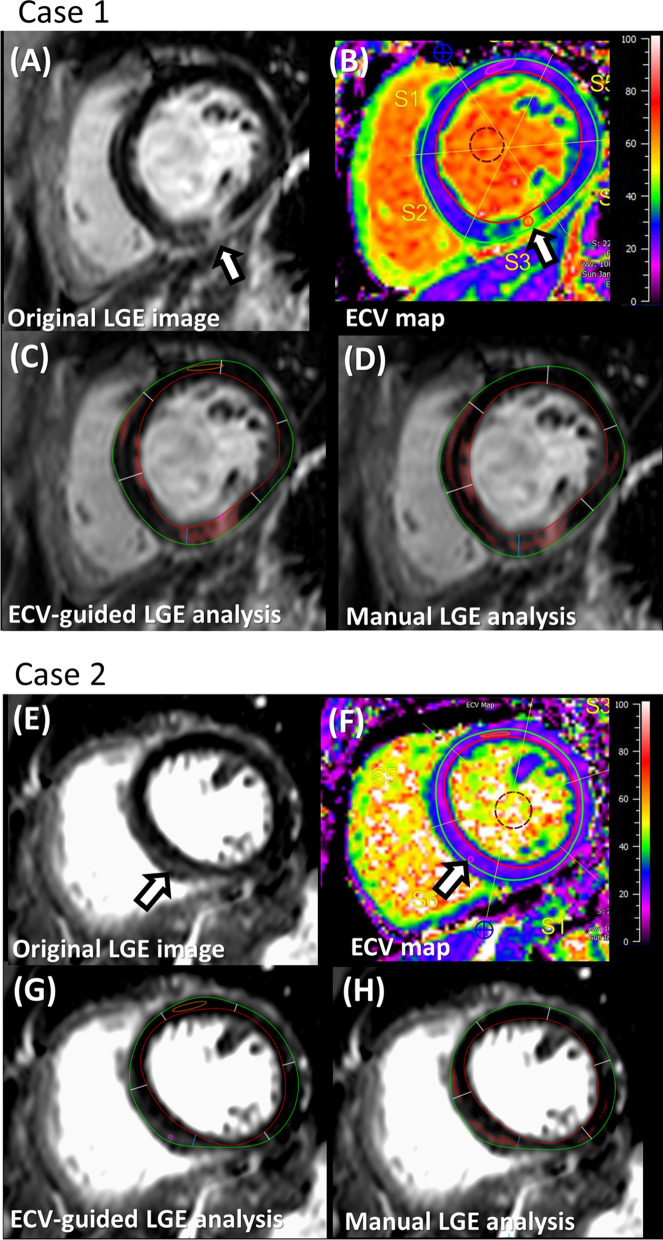
The non-ischemic groups were all female with the HIV positive rate of 73.8% (training) and 80% (validation). The ischemic group was all male with reduced LV function. An ECV cutoff of 31.5% achieved optimum performance (sensitivity: 90%, specificity: 86.7% in training; sensitivity: 100%, specificity: 81.8% in validation dataset). The identified n-SD threshold varied widely (range 3 SD-18 SD), and was independent of scar amount (β = -0.01, p = 0.92). In the non-ischemic cohorts, results suggested that the manual LGE assessment overestimated scar (%) in comparison to ECV-guided analysis [training: 4.5 (3.2-6.4) vs. 0.92 (0.1-2.1); validation: 2.5 (1.2-3.7) vs. 0.2 (0-1.6); P < 0.01 for both]. Intra- and inter-observer analyses of global scar (%) showed higher reproducibility in ECV-guided than manual analysis with CCC = 0.94 and 0.78 versus CCC = 0.86 and 0.73, respectively (P < 0.01 for all). In ischemic validation, the ECV-guided LGE analysis showed a comparable scar amount and reproducibility with the FWHM.
ECV-guided LGE analysis is a robust scar quantification method for a non-ischemic cohort. Trial registration ClinicalTrials.gov; NCT00000797, retrospectively-registered 2 November 1999; NCT02501811, registered 15 July 2015.
由于纤维化呈斑片状弥漫性分布,非缺血性心肌瘢痕的定量分析仍然是一项挑战。利用细胞外容积(ECV)指导延迟钆增强(LGE)分析或许能实现可靠的瘢痕评估。
前瞻性纳入三个队列,分别为80例非缺血性训练组、20例非缺血性验证组和10例缺血性验证组,并对其进行3.0特斯拉心脏磁共振成像检查。通过在训练队列中进行受试者工作特征曲线分析,比较左心室(LV)中部LGE最高信号强度(SI)区域的ECV值与视觉判定的LGE瘢痕有无情况,确定区分LGE瘢痕与非瘢痕的ECV临界值。基于该ECV临界值,在个体病例中优化LGE半自动阈值,使其比远心肌SI高n倍标准差(n-SD),以确保LGE图像与ECV图像对应。评估与手动测量(针对非缺血性病例)或半高宽(FWHM,针对缺血性病例)相比瘢痕量的方法间一致性。在随机选取的40例非缺血性和10例缺血性病例子集中研究观察者内和观察者间的可重复性。
非缺血性组均为女性,HIV阳性率分别为73.8%(训练组)和80%(验证组)。缺血性组均为男性,LV功能降低。ECV临界值为31.5%时性能最佳(训练组中敏感性为90%,特异性为86.7%;验证数据集中敏感性为100%,特异性为81.8%)。确定的n-SD阈值差异很大(范围为3 SD - 18 SD),且与瘢痕量无关(β = -0.01,p = 0.92)。在非缺血性队列中,结果表明与ECV指导分析相比,手动LGE评估高估了瘢痕(%)[训练组:4.5(3.2 - 6.4)对0.92(0.1 - 2.1);验证组:2.5(1.2 - 3.7)对0.2(0 - 1.6);两者P < 0.01]。观察者内和观察者间对整体瘢痕(%)的分析显示,ECV指导分析的可重复性高于手动分析,CCC分别为0.94和0.78,而手动分析的CCC分别为0.86和0.73(所有P < 0.01)。在缺血性验证中,ECV指导的LGE分析显示瘢痕量及可重复性与FWHM相当。
ECV指导的LGE分析是一种用于非缺血性队列的可靠瘢痕定量方法。试验注册ClinicalTrials.gov;NCT00000797,1999年11月2日追溯注册;NCT02501811,2015年7月15日注册。