Department of Urology, Fudan University Shanghai Cancer Center, No. 270 Dong an Road, Shanghai, 200032, People's Republic of China.
Department of Oncology, Shanghai Medical College, Fudan University, Shanghai, China.
BMC Cancer. 2021 Jul 27;21(1):857. doi: 10.1186/s12885-021-08603-z.
Primary urethral carcinoma (PUC) is a rare genitourinary malignancy with a relatively poor prognosis. The aim of this study was to examine the impact of surgery on survival of patients diagnosed with PUC.
A total of 1544 PUC patients diagnosed between 2004 and 2016 were identified based on the SEER database. The Kaplan-Meier estimate and the Fine and Gray competing risks analysis were performed to assess overall survival (OS) and cancer-specific mortality (CSM). The multivariate Cox regression model and competing risks regression model were used to identify independent risk factors of OS and cancer-specific survival (CSS).
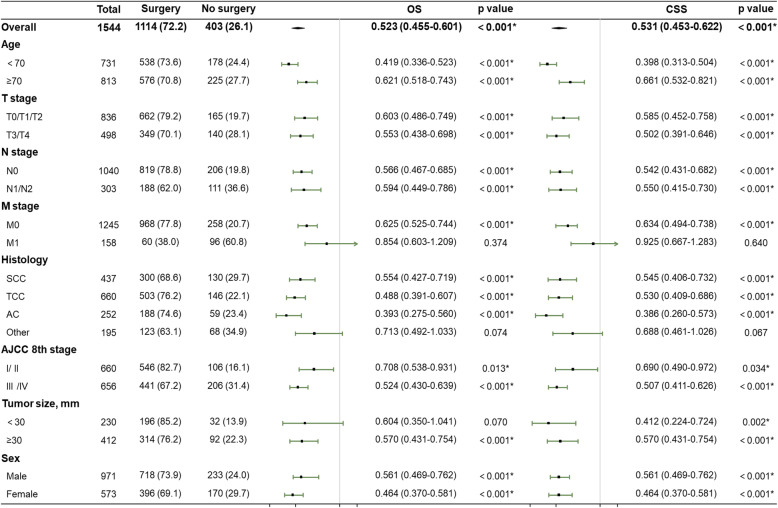
The 5-yr OS was significantly better in patients who received either local therapy (39.8%) or radical surgery (44.7%) compared to patients receiving no surgery of the primary site (21.5%) (p < 0.001). Both local therapy and radical surgery were each independently associated with decreased CSM, with predicted 5-yr cumulative incidence of 45.4 and 43.3%, respectively, compared to 64.7% for patients receiving no surgery of the primary site (p < 0.001). Multivariate analyses demonstrated that primary site surgery was independently associated with better OS (local therapy, p = 0.037; radical surgery, p < 0.001) and decreased CSM (p = 0.003). Similar results were noted regardless of age, sex, T stage, N stage, and AJCC prognostic groups based on subgroup analysis. However, patients with M1 disease who underwent primary site surgery did not exhibit any survival benefit.
Surgery for the primary tumor conferred a survival advantage in non-metastatic PUC patients.
原发性尿道癌(PUC)是一种罕见的泌尿生殖系统恶性肿瘤,预后相对较差。本研究旨在探讨手术对诊断为 PUC 患者生存的影响。
基于 SEER 数据库,共确定了 1544 例 2004 年至 2016 年期间诊断为 PUC 的患者。采用 Kaplan-Meier 估计和 Fine 和 Gray 竞争风险分析评估总生存率(OS)和癌症特异性死亡率(CSM)。采用多变量 Cox 回归模型和竞争风险回归模型确定 OS 和癌症特异性生存(CSS)的独立危险因素。
与未接受原发部位手术的患者(21.5%)相比,接受局部治疗(39.8%)或根治性手术(44.7%)的患者 5 年 OS 显著改善(p<0.001)。局部治疗和根治性手术均与 CSM 降低独立相关,预测 5 年累积发生率分别为 45.4%和 43.3%,而未接受原发部位手术的患者为 64.7%(p<0.001)。多变量分析表明,原发部位手术与 OS 改善独立相关(局部治疗,p=0.037;根治性手术,p<0.001)和 CSM 降低相关(p=0.003)。基于亚组分析,无论年龄、性别、T 分期、N 分期和 AJCC 预后组,均观察到类似的结果。然而,原发部位手术的 M1 期患者并未表现出任何生存获益。
对于非转移性 PUC 患者,手术治疗原发肿瘤可带来生存优势。